Cervical cancer: causes, detection, treatment and prevention
Comprehensive overview of cervical cancer: causes (HPV), signs, screening and diagnosis, treatments by stage, vaccination and public-health measures to reduce incidence and mortality.
Overview
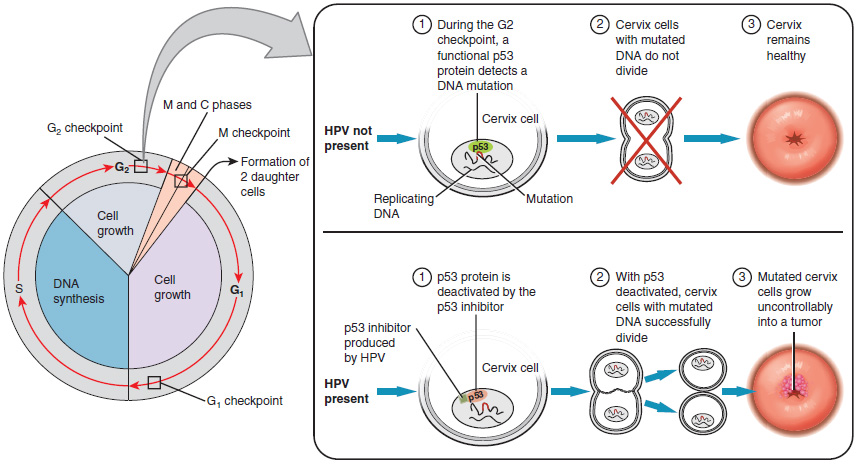
Cervical cancer develops in the cervix, the lower narrow part of the uterus that connects to the vagina. It is a form of malignancy most often driven by persistent infection with certain types of human papillomavirus (HPV). If undetected and untreated, invasive cervical cancer can cause serious illness and, in some cases, death. The natural history of most cases is slow progression from infection to precancer and, over years, to invasive disease, which is why prevention and early detection are effective.
Image gallery
10 Images






Causes and risk factors
Persistent infection with high-risk HPV types is the dominant cause. Other factors that increase the likelihood that an HPV infection will persist or progress include tobacco smoking, a weakened immune system (for example due to HIV), long-term use of oral contraceptives, having many full-term pregnancies, and early onset of sexual activity. Most HPV infections clear spontaneously, but a proportion can cause cellular changes that may develop into precancerous lesions.
Signs, screening, and diagnosis
Early cervical disease is frequently asymptomatic, which is why organized screening is central to prevention. When symptoms occur they may include abnormal vaginal bleeding (for example after sexual intercourse, between periods, or after menopause), unusual vaginal discharge, or pelvic pain. Because symptoms can be absent until advanced stages, regular screening with cytology (Pap test), HPV testing, or a combination is recommended in many settings; these approaches have substantially reduced incidence and mortality where they are widely applied.
Abnormal screening results are followed by diagnostic tests such as colposcopy and directed biopsy to confirm disease and determine the extent. Clinicians use test results and clinical examination to plan management and staging; timely diagnosis of precancerous lesions allows treatment that prevents progression to invasive cancer.
Treatment options
Treatment depends on the stage, size of lesion, and a person’s desire for future fertility. Precancerous changes are often treated with local procedures that remove or destroy abnormal tissue, such as loop electrosurgical excision or cone biopsy. Early invasive cancer can be managed surgically, ranging from fertility-sparing procedures to hysterectomy. For more advanced disease, radiotherapy combined with concurrent chemotherapy is a mainstay. Surgery and combined-modality care are planned by multidisciplinary teams. In selected advanced or recurrent cases, newer systemic and targeted treatments, including immunotherapy, are under study or used in specialist centres.
Prevention and vaccines
Primary prevention aims to prevent the HPV infections that lead to most cervical cancers. Licensed HPV vaccines protect against the HPV types responsible for the majority of cases; early vaccines prevented the types that cause about 70% of cancers, while more recent formulations cover additional oncogenic types and reduce a larger share of infections. Vaccination programs, when combined with screening, offer the strongest population-level protection. Safer-sex practices and smoking cessation also reduce risk.
Staging, prognosis and follow-up
Accurate staging guides treatment and helps predict outcomes. Prognosis depends largely on stage at diagnosis: early-stage disease treated appropriately has a much higher chance of cure than advanced-stage disease. After treatment for precancer or cancer, regular follow-up with clinical review and appropriate tests is important to detect recurrence or manage late effects.
Public-health impact and disparities
Cervical cancer remains a significant global health problem, particularly in regions with limited access to vaccination, screening, and timely treatment. Organized screening programs and widespread vaccination have changed disease patterns in many higher-resource settings, reducing both incidence and mortality. Efforts to expand access, strengthen health systems, and provide public education are central to reducing disparities.
- Key points: Persistent high-risk HPV infection is the main cause; most cases are preventable.
- Regular screening (Pap and/or HPV testing) and timely diagnosis reduce progression to invasive cancer.
- HPV vaccination, along with screening and risk reduction, offers the best prevention.
- Treatment is stage-dependent and may include local excision, surgery, radiotherapy, and chemotherapy.
For more information on anatomy and how cervical disease develops, see resources on the cervix and the uterus. Guidance about symptoms and what to do if you have concerns is available via general information pages on symptoms. If you or someone you care for needs clinical advice about screening intervals, vaccination eligibility, or treatment choices, consult a healthcare professional or local clinical guidelines. Patient support and specialist services can be found through vaccination and public-health links such as those about cervical cancer prevention and bleeding evaluation.
Reliable resources and national programs vary by country; check local recommendations and services for up-to-date schedules, referral pathways, and support options.
Related articles
Author
AlegsaOnline.com Cervical cancer: causes, detection, treatment and prevention Leandro Alegsa
URL: https://en.alegsaonline.com/art/18229
Sources
- fda.gov : "FDA Licenses New Vaccine for Prevention of Cervical Cancer"
- jci.org : "Prophylactic human papillomavirus vaccines"
- doi.org : 10.1172/JCI28607
- pubmed.ncbi.nlm.nih.gov : 16670757