Rheumatic fever: causes, signs, diagnosis and prevention
Rheumatic fever is an immune-mediated inflammatory illness that can follow untreated strep throat. It affects the heart, joints, skin and nervous system and can cause long-term valve damage.
Overview
Rheumatic fever is an immune-mediated inflammatory illness that typically develops after infection with group A streptococci. It most often affects children and adolescents and may cause transient or lasting damage to cardiac valves, joints, skin and the nervous system. Early recognition and treatment of streptococcal throat infections reduces the risk.
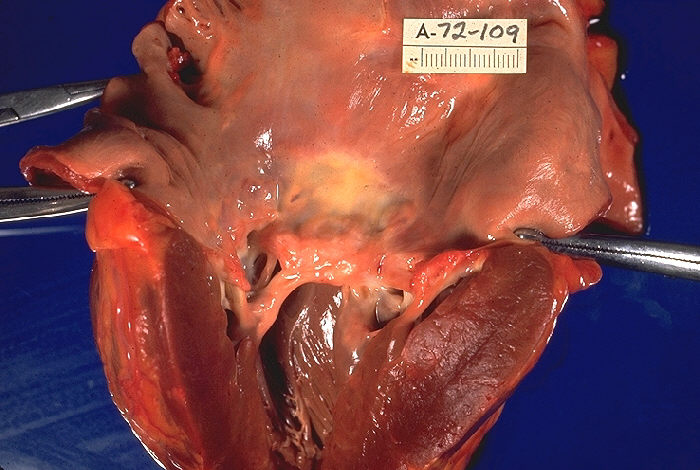
Image gallery
5 Images



Cause and mechanism
The condition arises when the body’s immune response to a streptococcal throat infection cross-reacts with human tissues (a process often called molecular mimicry). The autoimmune reaction can target the heart, joints, skin and central nervous system, producing inflammation that underlies the clinical features.
Main clinical features
Presentation varies. Some patients have acute carditis with murmurs and heart failure; others have migratory arthritis, characteristic skin rashes, subcutaneous nodules or neurological symptoms. Classic major manifestations (the Jones criteria) include:
- Carditis (inflammation of the heart)
- Polyarthritis (migratory joint pain and swelling)
- Sydenham's chorea (involuntary movements)
- Erythema marginatum (ring-shaped rash)
- Subcutaneous nodules
Diagnosis and treatment
Diagnosis is clinical, supported by evidence of recent streptococcal infection (throat culture, rapid tests or antibody titers) and imaging such as echocardiography to assess valve involvement. Treatment combines eradication of the bacteria (usually with penicillin), anti-inflammatory therapy (aspirin or corticosteroids in some cases), supportive care including rest, and long-term secondary prophylaxis to prevent recurrences. In advanced cases with severe valve damage, surgical repair or replacement may be required.
Epidemiology, prevention and public health
Rheumatic fever has declined in many high-income countries but remains an important cause of heart disease in parts of the world where access to prompt diagnosis and antibiotics is limited. It is relatively more common in regions such as the Middle East, eastern Europe, South America and the Far East, and is much rarer in much of western Europe and North America. Primary prevention focuses on treating streptococcal pharyngitis promptly; secondary prevention uses regular antibiotic prophylaxis for those with prior rheumatic fever to prevent recurrence.
History and notable facts
Rates of rheumatic fever fell dramatically in the 20th century with improved living conditions and routine use of antibiotics, but the disease still causes significant morbidity where care is limited. Some historical figures have been retrospectively suggested to have suffered from rheumatic fever, which can leave lasting valve damage known as rheumatic heart disease. Ongoing public health efforts and research into vaccines against group A streptococcus aim to reduce the global burden.[LINKS]
References and further reading are available through specialist clinical resources and public health organizations; for introductory material see links provided above.
inflammatory | group A streptococci | heart | skin | joints | central nervous system | Middle East | eastern Europe | South America | Far East | North America
Related articles
Author
AlegsaOnline.com Rheumatic fever: causes, signs, diagnosis and prevention Leandro Alegsa
URL: https://en.alegsaonline.com/art/82497