Iron-deficiency anemia: causes, symptoms, diagnosis, treatment, and prevention
Comprehensive overview of iron-deficiency anemia: causes, mechanisms, risk groups, symptoms, diagnosis, treatment options, prevention, public-health aspects and when to seek care.
Overview
Iron-deficiency anemia is a common form of anemia that results when the body lacks sufficient iron to make normal amounts of hemoglobin, the oxygen-carrying component of red blood cells. It is the most frequent nutritional anemia worldwide and may cause fatigue, reduced exercise tolerance and impaired cognitive or work performance. For general background on related disorders see anemia and for information on iron in food and diet see dietary iron.
Image gallery
10 Images








Causes and mechanisms
Three main processes underlie iron deficiency: inadequate intake, impaired absorption, and excessive loss. Inadequate intake occurs when dietary iron is low or when foods with low bioavailability form the main diet. Impaired absorption can arise from gastrointestinal diseases, intestinal surgery, or interactions with other nutrients or medications. Excessive loss most commonly results from chronic bleeding, for example from menstruation or gastrointestinal lesions; see bleeding and menstruation as common contributors.
- Insufficient dietary iron affects infants, young children, pregnant people and those on restrictive diets.
- Malabsorption from conditions such as celiac disease, inflammatory bowel disease or after gastric bypass surgery.
- Blood loss due to ulcers, cancers, heavy menstrual bleeding, or parasitic infections.
Pathophysiology and risk groups
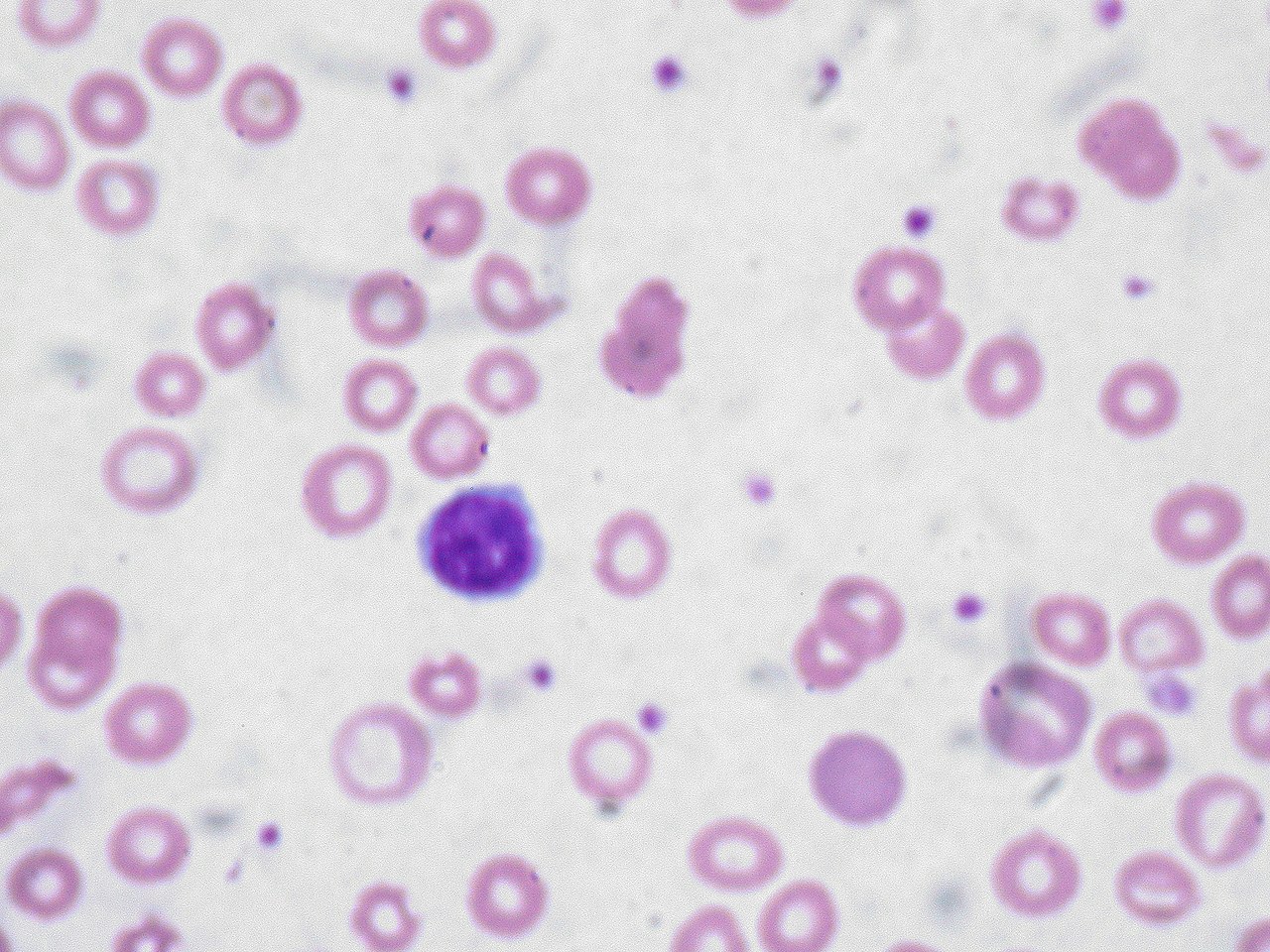
When iron stores fall, the body first draws on stored iron; with persistent deficit, production of hemoglobin declines and red blood cells become smaller and paler. Risk groups include women of reproductive age, pregnant people because of increased iron needs, infants and young children during periods of rapid growth, and older adults where chronic disease or blood loss may be a factor. Premature infants and those with low birth weight have reduced iron stores at birth and are especially vulnerable.
Signs and symptoms
Symptoms develop gradually and may be subtle. Typical symptoms are general tiredness, weakness, reduced stamina, and shortness of breath on exertion. Physical findings can include pallor of the skin and mucous membranes; more specific complaints may include dizziness, palpitations, brittle nails, and unusual cravings for non-food items (pica). For common symptom descriptions see symptoms, pale appearance at pallor, and general tiredness at tiredness.
Diagnosis
Diagnosis relies on blood tests. A complete blood count may show a low hemoglobin concentration and characteristic small, pale red cells. Additional tests such as serum ferritin (a marker of iron stores), transferrin saturation and other iron indices help confirm iron deficiency and exclude other causes. Inflammatory states can affect some tests, so clinical interpretation may require several measurements and clinical correlation; see clinical testing guidance at diagnosis. The key laboratory value, hemoglobin, is discussed at hemoglobin.
Treatment
Management has two linked aims: correct the anemia and identify and treat the underlying cause. Oral iron supplements are the first-line treatment for many people and are effective when absorption is adequate and side effects are manageable. Intravenous iron is used when oral iron is not tolerated, not effective, or when rapid replenishment is required. In severe cases or when there is ongoing significant blood loss, transfusion or targeted surgical or endoscopic treatment may be necessary.
- Dietary advice: encourage iron-rich foods and factors that enhance absorption (for example vitamin C) and avoid inhibitors around meals.
- Supplementation: follow medical advice on dosing and duration; therapy often continues until iron stores are restored.
- Address causes: investigate sources of bleeding, screen for gastrointestinal lesions, treat heavy menstrual bleeding and manage malabsorption.
Prevention and public-health approaches
Prevention combines individual advice and population measures: dietary education, targeted supplementation for at-risk groups (such as pregnant people and young children), and food fortification programs in some regions. Public-health measures also aim to reduce infections and parasitic diseases that cause blood loss and to improve access to reproductive and primary health services.
Epidemiology and global patterns
Iron-deficiency anemia affects a large portion of the global population. Prevalence is higher where diets are less varied, healthcare access is limited, or infections that cause blood loss are common. It disproportionately affects women of reproductive age and young children. Regions with a notable burden include parts of Central Africa and Latin America; regional references in broad surveys include Central Africa, Brazil, Asia, Central America, and Eastern Europe, while lower rates are typically reported in North America.
Complications, prognosis and special considerations
If untreated, iron-deficiency anemia can impair quality of life and, in severe cases, contribute to cardiac strain and complications in pregnancy such as increased risk of preterm delivery. Most people recover fully with appropriate treatment, but recurrence is possible if the underlying cause is not addressed. Special attention is given to pregnant people, infants and the elderly because of differing causes, consequences and treatment needs.
If you suspect iron-deficiency anemia, consult a healthcare professional for appropriate testing and personalised management rather than self-diagnosing. For introductory reading see anemia overview and for clinical guidance on testing and management see diagnostic guidance.
Related articles
Author
AlegsaOnline.com Iron-deficiency anemia: causes, symptoms, diagnosis, treatment, and prevention Leandro Alegsa
URL: https://en.alegsaonline.com/art/48210
Sources
- jn.nutrition.org : Review of numbers of infections