1918 Influenza Pandemic (Spanish flu)
Worldwide outbreak of influenza from 1918–1920 that infected roughly one quarter of people and caused tens of millions of deaths; notable for its high mortality among young adults and lasting global impact.
Overview
The 1918 influenza pandemic, commonly called the Spanish flu, was a global outbreak of influenza that occurred in the closing years of World War I and the immediate aftermath. Contemporary and later estimates suggest the pandemic began in January 1918 and continued in successive waves until about December 1920. It infected an estimated 500 million people worldwide at a time when the global population was roughly 1.8 billion, and caused an estimated 50–100 million deaths, making it one of the deadliest events in human history. The term "Spanish flu" arose because neutral Spain reported openly on the disease while wartime censorship masked the scale of illness in combatant countries.
Image gallery
10 Images








Epidemiology and clinical features
The causative agent was an influenza A virus of the H1N1 subtype, a form of influenza. Unlike typical seasonal influenza, which disproportionately kills the very young and the elderly, the 1918 pandemic displayed an unusual mortality curve that produced high death rates in otherwise healthy young adults. Modern analyses of preserved tissues indicate that severe cases often involved an extreme inflammatory reaction, described in the scientific literature as a cytokine storm, in which the host immune system mounted an excessive response that damaged the body. Secondary bacterial pneumonia was also a major immediate cause of death.
Origins, spread and wartime context
The geographic origin of the pandemic remains uncertain and is still debated among historians and epidemiologists. There is limited and sometimes contradictory epidemiological evidence about the earliest cases. Wartime conditions—troop movements, crowded military camps and transport—helped the virus move rapidly between continents. Reporting was distorted by wartime censorship and restrictions on the press in countries such as Germany, Britain and France, while newspapers in neutral Spain and elsewhere published more freely. The disease reached the Pacific islands and the Arctic, demonstrating the speed and breadth of global transmission. It also seriously affected troops and civilian populations in the United States.
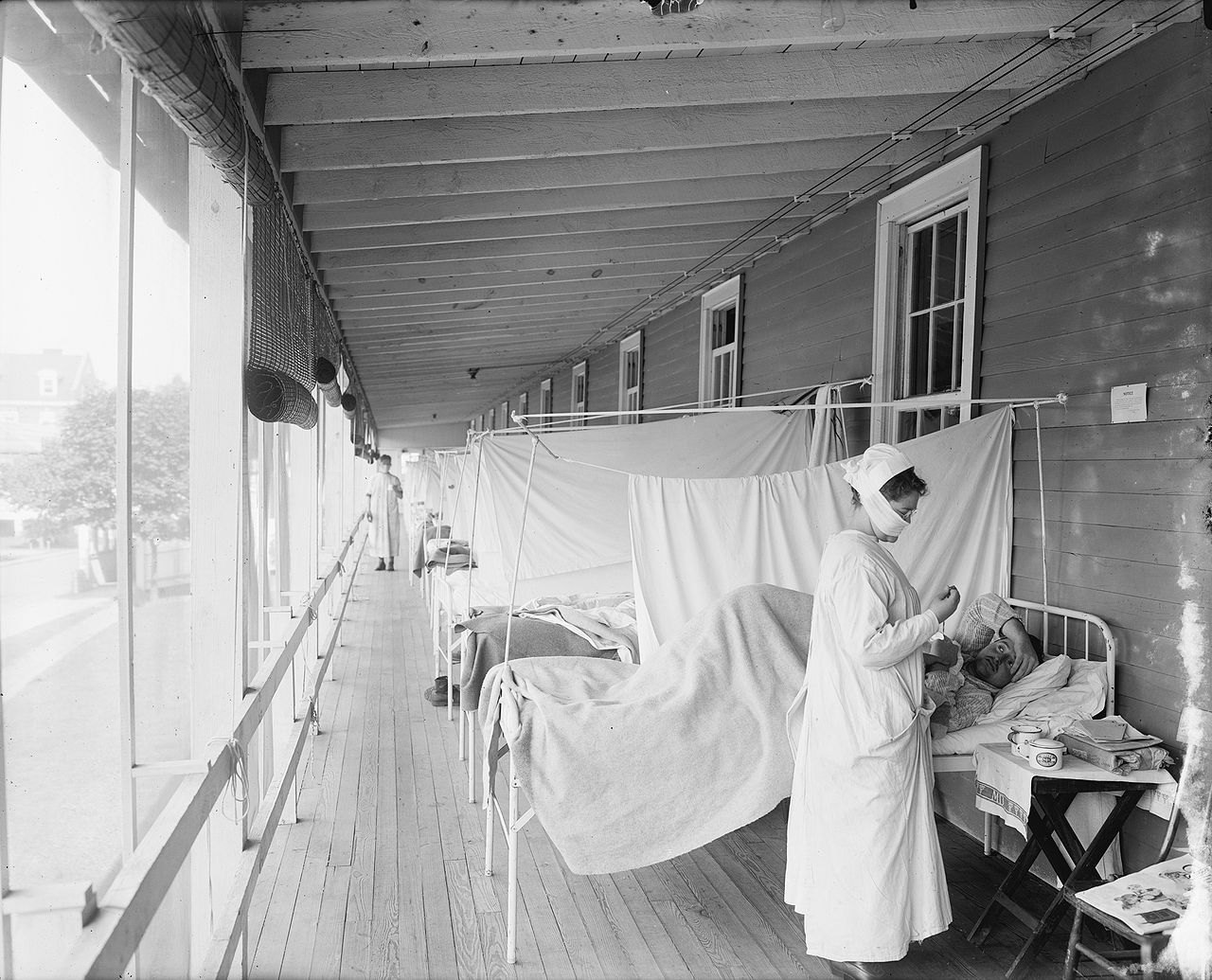
Public health responses and social impact
Communities used non-pharmaceutical interventions similar to those recommended today: isolation of cases, closing schools and theaters, banning public gatherings, and encouraging mask use. Local public health authorities implemented quarantine, travel restrictions and sanitation measures, with varying degrees of success. The pandemic disrupted economies, strained medical services and influenced wartime morale and politics. Social effects included labor shortages, interruptions to commerce and changes in public health organization that endured after the crisis.
Research, legacy and later pandemics
Decades of study—ranging from archival research to laboratory analysis of preserved tissue and exhumed samples—identified the 1918 virus as an H1N1 influenza A strain and clarified aspects of its pathology. These studies helped explain the unusual age profile of fatalities and contributed to pandemic preparedness planning for later outbreaks. Scholars have explored possible links between the 1918 pandemic and subsequent neurological syndromes such as encephalitis lethargica, though causal connections remain uncertain. Comparisons are often drawn with later pandemics, including a 21st-century outbreak caused by a novel H1N1 strain beginning in North America (2009 H1N1 pandemic), and with regional influenza outbreaks and epidemics (influenza outbreaks).
Notable facts and distinctions
- The pandemic infected an unusually large proportion of the global population and caused mortality on an unprecedented scale. See analyses of the 1918 pandemic and its global burden.
- Its pattern of high mortality among healthy young adults is attributed in part to immune overreaction; studies reference immune responses and the immune system in this context.
- The historic record was shaped by political factors: press controls and differing national responses changed public perception and led to the nickname tied to Spain.
- The disease spread across continents and to remote regions, including island and polar communities (Pacific, Arctic), and affected both civilian and military populations (United States, European combatant states).
- Ongoing research draws on archival material and biomedical methods to refine estimates and to inform modern preparedness; scholars caution about gaps in data and the limits of retrospective diagnosis.
For more detailed timelines, archival documents and scientific overviews consult specialized histories and public health resources, and follow primary-source collections and modern reviews of the pandemic. Historical inquiry continues into possible early locations such as North America and other proposed sites, including references to outbreaks in places like Mexico, and the broader lessons for managing future global health emergencies.
Further reading and resources are available through institutional and subject-specific portals; examples of research portals and curated summaries can be found via links to historical archives and medical reviews (chronologies, demographic studies, and population analyses), and through scientific syntheses addressing pathogenesis (cytokine research) and long-term societal effects (global implications, historical context).
Note: this article synthesizes broadly accepted findings while avoiding speculation about unresolved details. For primary sources and up-to-date scientific work consult specialist publications and public health agencies (biomedical literature, policy analyses, archival accounts, and dedicated historical studies linked above).
Related articles
Author
AlegsaOnline.com 1918 Influenza Pandemic (Spanish flu) Leandro Alegsa
URL: https://en.alegsaonline.com/art/47297
Sources
- wwwnc.cdc.gov : "1918 Influenza: The Mother of All Pandemics"
- doi.org : 10.3201/eid1201.050979
- darwin.nap.edu : "1: The Story of Influenza"
- census.gov : "Historical Estimates of World Population"
- pubmed.ncbi.nlm.nih.gov : 2021692
- virus.stanford.edu : "The Influenza Pandemic of 1918"
- doi.org : 10.1353/bhm.2002.0022
- pubmed.ncbi.nlm.nih.gov : 11875246
- npr.org : "Origins of the 1918 Pandemic: The Case for France"
- eurekalert.org : "Analysis of Spanish flu cases in 1918–1920 suggests transfusions might help in bird flu pandemic"
- popularmechanics.com : "Spanish Flu Pandemic: 1918"
- ncbi.nlm.nih.gov : "Into the Eye of the Cytokine Storm"
- doi.org : 10.1128/MMBR.05015-11
- linkinghub.elsevier.com : "Children and encephalitis lethargica: A historical review"
- doi.org : 10.1016/j.pediatrneurol.2007.04.012