Gallbladder cancer: overview, risks, diagnosis and treatment
A concise, neutral overview of gallbladder cancer: what it is, where it is more common, typical signs, how it is diagnosed and treated, and important risk factors and outcomes.
Overview
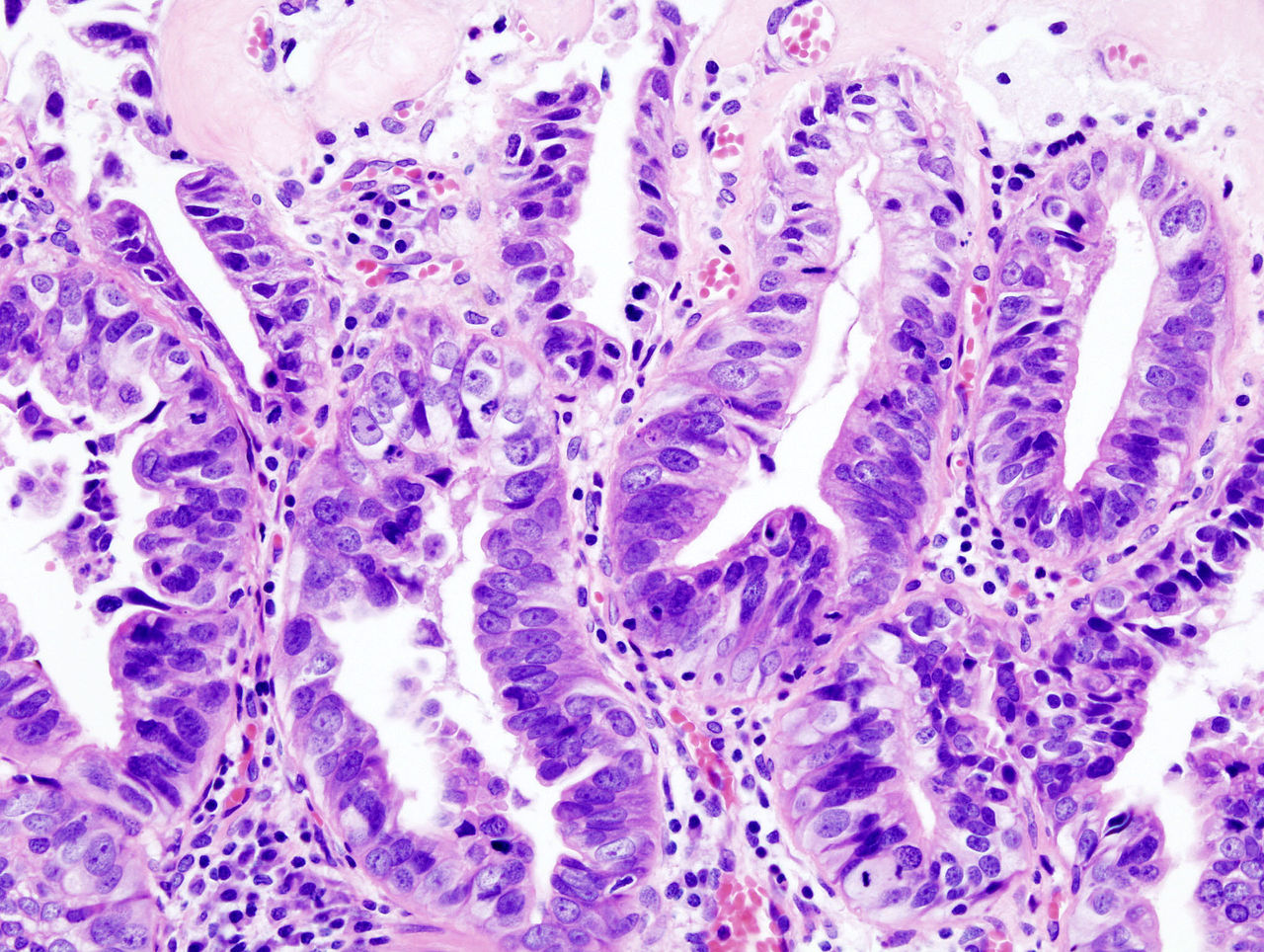
Gallbladder cancer is an uncommon malignancy that originates in the epithelial lining of the gallbladder. Tumors most often arise as adenocarcinomas and may range from carcinoma in situ to deeply invasive disease. Because early symptoms are subtle or absent, many cases are discovered late or incidentally during imaging or after gallbladder surgery.
Image gallery
3 Images

Geography and risk groups
The incidence varies markedly by region and population. It is more frequently reported in parts of central and South America, central and eastern Europe, China, Japan and northern India. Certain ethnic groups show higher rates, including some Native American communities and people of Hispanic or South Asian background. Age, female sex, and chronic gallbladder conditions are consistent risk correlates.
Causes, characteristics and spread
Persistent inflammation of the gallbladder — especially related to long-standing gallstones or gallbladder polyps — is linked to malignant transformation. Tumors may invade adjacent structures, notably the liver, and can extend to lymph nodes and distant sites. Obstructive features such as jaundice often indicate biliary involvement; spread to other organs is common in advanced stages (metastasis).
Signs, symptoms and diagnosis
- Common symptoms: upper abdominal or right-sided pain, nausea, weight loss, jaundice, or a palpable mass.
- Diagnosis relies on imaging (ultrasound, CT, MRI) and endoscopic techniques; tissue confirmation by biopsy is used when feasible.
- Occasionally the tumor is found incidentally in a gallbladder removed for presumed benign disease.
Treatment and prognosis
Surgery offers the only chance for cure when the disease is detected early. Options range from simple cholecystectomy for very early lesions to extended resections that remove part of the liver and regional lymph nodes for more advanced local disease. When complete resection is not possible, chemotherapy and radiotherapy can provide palliation, and selected patients may be offered systemic regimens or clinical trials. Overall outcomes are better for small, localized tumors; prognosis worsens with vascular invasion, nodal involvement or distant metastases.
Prevention, surveillance and notable facts
Reducing modifiable risks includes managing symptomatic gallstones and monitoring large gallbladder polyps. In regions or populations with high incidence, clinicians may have a lower threshold for investigation. Important practical points: many gallbladder cancers are adenocarcinomas, early removal can be curative, and presentation differs from more common biliary or hepatic tumors. Research continues into molecular targets and improved early detection strategies.
For further reading and clinical guidelines, consult specialist resources and local oncology services.
Related articles
Author
AlegsaOnline.com Gallbladder cancer: overview, risks, diagnosis and treatment Leandro Alegsa
URL: https://en.alegsaonline.com/art/37306
Sources
- pubmed.ncbi.nlm.nih.gov : 14606770
- ncbi.nlm.nih.gov : "Gallstones and the risk of biliary tract cancer: a population-based study in China"
- doi.org : 10.1038/sj.bjc.6604047
- pubmed.ncbi.nlm.nih.gov : 18000509
- ispub.com : "Incidence of gall bladder cancer in rural and semiurban population of north central India: A first insight"