Gastritis: causes, symptoms, diagnosis and management
Gastritis is inflammation of the stomach lining. This article explains causes, common symptoms, diagnostic approaches, treatment options and prevention, with practical distinctions and notable facts.
Gastritis refers to inflammation of the stomach lining. The condition ranges from a short-lived irritation to chronic inflammation that may damage the mucosal surface and affect digestion. The word describes a pattern of injury rather than a single disease, and many different factors can trigger the inflamed state. For a general definition see inflammation and for the affected organ see stomach.
Image gallery
4 Images


Causes and risk factors
Gastritis has multiple causes; some are temporary and others are long-term. Common contributing factors include:
- Medications that impair the stomach’s protective lining, especially long-term use of nonsteroidal anti-inflammatory drugs such as aspirin and ibuprofen.
- Acute stressors on the body after major surgery, severe injury, burn injuries, or serious infections (including systemic infections) referenced at infections.
- Infectious causes: bacterial colonization, most notably bacteria such as Helicobacter pylori, can produce chronic gastritis.
- Immune-related disease: autoimmune gastritis and conditions like pernicious anemia that reduce intrinsic factor and vitamin B12 absorption.
- Other contributors: chronic bile reflux, excessive alcohol intake, smoking, and some systemic illnesses.
Typical symptoms
Many people with gastritis have mild or no symptoms. When present, symptoms are often nonspecific and overlap with other digestive disorders. Frequent complaints include:
- Abdominal pain, usually a burning or gnawing sensation in the upper abdomen.
- Indigestion, early fullness and bloating.
- Nausea and sometimes vomiting.
- A feeling of fullness after small meals, loss of appetite, or belching.
Diagnosis
Diagnosis combines clinical history, physical examination and tests. Physicians will ask about medication use, alcohol intake, recent illnesses, and autoimmune conditions. Common diagnostic tools include:
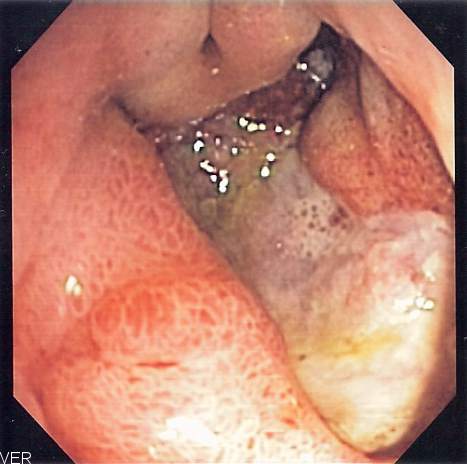
- Endoscopy with visual inspection and biopsy to assess inflammation, erosions, or atrophy.
- Blood tests to check for anemia, inflammation markers, and antibodies in autoimmune cases.
- Stool tests or breath tests for H. pylori detection, and sometimes urea breath tests or culture.
Treatment and management
Treatment aims to remove or reduce the cause, relieve symptoms, and promote healing. Approaches are tailored to the underlying trigger and may include:
- Avoiding or replacing irritating medications and limiting alcohol and tobacco.
- Acid-suppressing medications such as proton pump inhibitors or H2 blockers to permit mucosal repair.
- Eradication therapy (antibiotics plus acid suppression) when H. pylori is present.
- Over-the-counter agents like antacids for symptom relief and supportive measures such as dietary changes to avoid trigger foods.
- Specific treatment for autoimmune or deficiency states — for example, vitamin B12 replacement when related to pernicious anemia.
Prevention and complications
Prevention focuses on minimizing risk: use NSAIDs only as directed, limit alcohol, treat infections promptly, and manage chronic medical conditions. Untreated chronic gastritis can lead to complications such as peptic ulcers, gastrointestinal bleeding or, in some long-standing cases, mucosal atrophy that interferes with digestion and nutrient absorption. Early medical evaluation for persistent upper abdominal symptoms helps reduce the risk of progression.
For concise guidance and further reading on related topics see resources about inflammation, medication safety including aspirin and ibuprofen, surgical recovery risks, infectious causes overview, bacterial agents information, diagnostic methods for Helicobacter pylori, and practical notes on abdominal pain, indigestion, nausea, vomiting and the role of common remedies like antacids.
Related articles
Author
AlegsaOnline.com Gastritis: causes, symptoms, diagnosis and management Leandro Alegsa
URL: https://en.alegsaonline.com/art/37694
Sources
- umm.edu : "Gastritis"
- merck.com : "Gastritis"
- digestive.niddk.nih.gov : "Gastritis"
- wrongdiagnosis.com : "Gastritis: Diagnostic Tests for Gastritis"
- webmd.com : "What is Gastritis?"