Knee (joint) — anatomy, function, common problems and care
Overview of the knee joint: major bones and soft tissues, biomechanics, typical injuries and treatments, and practical tips for prevention and rehabilitation.
Overview
The knee is the principal joint that connects the upper and lower segments of the leg and bears a large portion of the body's weight. Often described as a complex hinge, the knee joint allows flexion and extension with limited rotation when flexed. Its stability and mobility arise from the coordinated interaction of bones, ligaments, cartilage, and muscles acting together to support standing, walking, running and jumping.
Image gallery
10 Images








Anatomy and main components
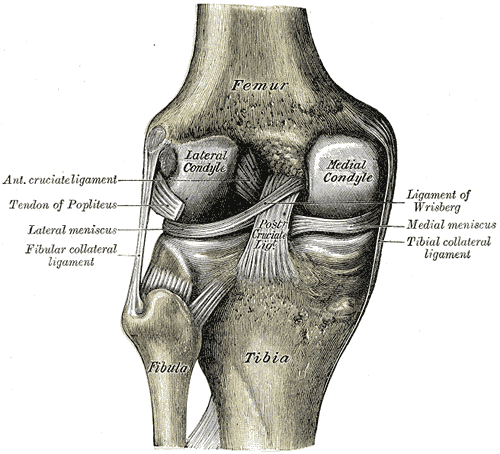
Structurally, the knee links several bones and many supporting tissues. The major bones involved are the group referred to as the long bones of the leg, including the femur (thigh bone), the tibia (shin bone) and the fibula, together with the sesamoid patella (kneecap). A network of ligaments provides passive stability while surrounding muscles and tendons supply active control. The knee surfaces are covered by articular cartilage, and two crescent-shaped menisci sit on the tibial plateau to distribute load and absorb shock.
How it works: movement and lubrication
Functionally the joint permits bending and straightening with small amounts of rotation and translation that allow the foot and lower leg to orient during gait. Although often called a hinge, the knee is more accurately a modified hinge that relies on complex geometry and soft tissue tension to permit smooth motion. A synovial membrane secretes fluid that lubricates the surfaces and nourishes cartilage, reducing friction and wear during repeated cycles of loading.
Common injuries and conditions
Knee problems arise from acute trauma, repetitive stress, degeneration, or developmental factors. Frequent issues include:
- Ligament sprains and tears (for example anterior cruciate ligament or ACL), often from twisting or direct impact; the ligaments are the principal stabilizers of the knee (ligaments).
- Meniscal tears, where the crescent cartilages become damaged by rotation or degeneration; the menisci are a key part of the knee's shock-absorbing system (meniscus and cartilage).
- Patellofemoral pain and instability, related to tracking of the kneecap over the femur (femur and patella interactions).
- Osteoarthritis, a wear-related breakdown of articular cartilage causing pain and stiffness, more common with age and prior injury.
- Overuse syndromes that affect tendons and bursae, often seen in athletes or people with repetitive knee loading (leg mechanics are a contributing factor).
Diagnosis, treatment and rehabilitation
Evaluation begins with a history and physical examination and may include imaging studies. Management ranges from conservative measures — rest, activity modification, physical therapy to strengthen the muscles and improve alignment — to procedures such as arthroscopy or joint replacement for severe degeneration. Surgical repair or reconstruction is sometimes indicated for unstable ligament injuries. Rehabilitation emphasizes restoring range of motion, strength and gradual return to function while protecting healing tissues.
Prevention and notable facts
Preventive measures include strengthening hip and thigh muscles, improving movement patterns and using appropriate footwear. Weight management reduces chronic load. Because the knee combines mobility with weight-bearing responsibility, small changes in alignment or muscle balance can greatly influence risk of injury and progression of wear. For more technical references and clinical guidance, see resources on joint mechanics and orthopedics (bones, tibia, fibula, hinge-like mechanics, knee joint overview).
Related articles
Author
AlegsaOnline.com Knee (joint) — anatomy, function, common problems and care Leandro Alegsa
URL: https://en.alegsaonline.com/art/53970