Subdural hematoma: causes, presentation, diagnosis and management
Subdural hematoma (SDH) is blood collecting between the dura and arachnoid layers of the meninges, usually after head injury. This article explains causes, symptoms, diagnosis, treatment and outcomes.
Overview
A subdural hematoma (SDH) is a collection of blood that accumulates between the dura mater and the arachnoid mater of the meninges surrounding the brain. It most commonly follows head trauma such as a traumatic brain injury, but can also develop with minor or unrecognized blows in people who take blood thinners or in older adults whose brain shrinks slightly with age. The bleeding usually arises from torn bridging veins, which lie in the subdural space and bleed at venous pressure.
Image gallery
4 Images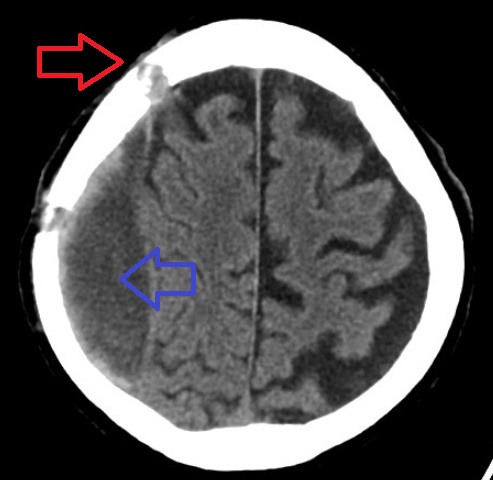



Causes and mechanism
Bridging veins span from the cortical surface to the dural sinuses; shearing forces during acceleration-deceleration injuries can tear these veins. SDH is classified by timing: acute (symptoms within 72 hours), subacute (days to two weeks), and chronic (weeks to months). Chronic subdural hematomas may form when slow venous bleeding allows blood to liquefy and enlarge over time.
Clinical presentation
Symptoms often depend on the size, rate of bleeding and patient factors. Acute hematomas can produce rapid deterioration, while chronic hematomas may cause progressive, subtle complaints. Typical features include:
- Headache and confusion
- Focal neurologic deficits such as weakness or speech difficulty
- Sensory changes, drowsiness, or reduced level of consciousness
- Seizures or behavioral changes
Because venous bleeding is slower than arterial, signs and symptoms may be delayed and develop over days to weeks.
Diagnosis and treatment
Computed tomography (CT) is the usual first-line imaging study and detects acute blood quickly; magnetic resonance imaging (MRI) may better characterize chronic collections. Small, asymptomatic hematomas can be observed with serial imaging and medical management, while large or symptomatic hematomas often require neurosurgical drainage. Options include burr-hole drainage for liquefied chronic hematomas or craniotomy for acute, clotted collections. Management also addresses intracranial pressure, seizure risk and reversal of anticoagulation when appropriate.
Prognosis and prevention
Outcomes vary. Factors that influence recovery include age, level of consciousness at presentation, hematoma size and midline shift on imaging, and speed of treatment. Preventive measures focus on fall prevention, cautious use of anticoagulant medications, and protective headgear in high-risk activities.
Notable distinctions
SDH is distinct from epidural hematoma (bleeding between the skull and dura, often arterial and rapid) and intracerebral hemorrhage (bleeding within brain tissue). Recognizing the pattern of injury, timing of symptoms and imaging features helps guide urgent management and prognosis.
For more general background on head injury, anatomy of the meninges, brain function, and symptom lists, see resources linked here: traumatic brain injury, meninges, brain, symptoms.
Related articles
Author
AlegsaOnline.com Subdural hematoma: causes, presentation, diagnosis and management Leandro Alegsa
URL: https://en.alegsaonline.com/art/94472
Sources
- nlm.nih.gov : "Subdural hematoma : MedlinePlus Medical Encyclopedia"