Coronary artery bypass surgery (CABG)
Surgical treatment for blocked coronary arteries that restores blood flow to the heart by grafting vessels from elsewhere on the body; commonly called CABG or heart bypass.
Coronary artery bypass surgery, commonly called coronary artery bypass grafting or CABG (pronounced "cabbage"), is an operation that improves blood supply to the heart muscle by creating new routes around blocked coronary arteries. It relieves angina (chest pain) caused by reduced blood flow, can improve quality of life and, for selected patients, may reduce the risk of heart attack or death from coronary artery disease. See general procedure information: coronary artery bypass surgery.
Image gallery
10 Images








How CABG works and common grafts
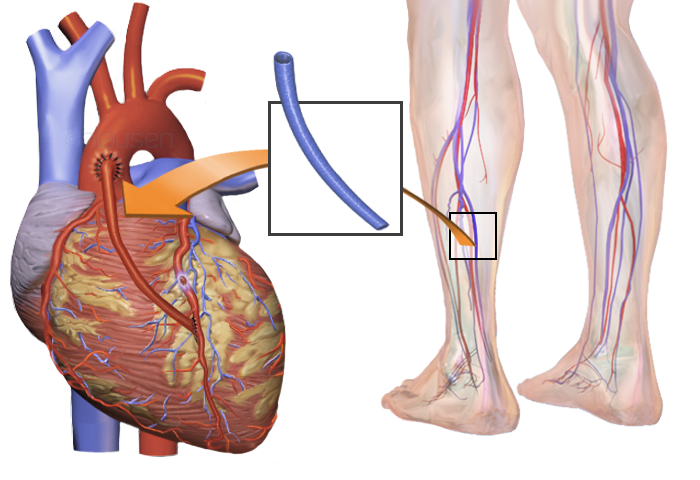
The surgeon takes blood vessels from another part of the body and attaches them to the coronary arteries beyond blockages, so blood can bypass narrowed sections. Typical conduits include:
- Internal thoracic (mammary) artery — often the preferred arterial graft for the left anterior descending artery because of long-term durability.
- Saphenous vein — taken from the leg and commonly used for multiple bypasses; veins may have lower long-term patency than arterial grafts.
- Radial artery — taken from the forearm and used when an arterial conduit is desirable.
For background on why restoring flow matters, see resources on reduced coronary perfusion: lack of blood flow, and on related symptoms such as chest pain: angina and chest pain.
Procedure types and surgical technique
Traditional CABG is performed with the heart temporarily stopped while a heart–lung machine (cardiopulmonary bypass) maintains circulation and oxygenation. This permits a still surgical field and multiple grafts. An alternative, called "off‑pump" CABG, is done while the heart is still beating using stabilizing devices; it may reduce certain complications in selected patients. Minimally invasive and hybrid approaches combine smaller incisions, robotic assistance, or percutaneous coronary interventions to tailor treatment to patient needs.
Indications, benefits and risks
CABG is usually recommended for patients with severe or multivessel coronary artery disease, significant left main coronary artery narrowing, or when symptoms persist despite medical therapy or after failed stenting. Benefits include relief of angina, improved exercise tolerance and, in some anatomies, improved survival. Risks vary with patient health and procedure complexity and can include wound infection, bleeding, stroke, heart attack, kidney problems and graft failure. Patients and clinicians weigh long‑term graft patency, comorbidities and recovery time when choosing CABG versus other therapies. Helpful further reading on heart disease outcomes: heart disease and risk.
History and outcomes
Modern coronary bypass techniques developed in the mid‑20th century. Early advances in heart–lung machines made on‑pump surgery possible; surgical teams later refined graft choices and operative strategies. A landmark development was the routine use of saphenous vein grafts and arterial grafting, which evolved into today’s mix of conduits. Long‑term outcomes depend on graft type, patient adherence to secondary prevention (lipid control, blood pressure, smoking cessation) and follow‑up care.
Aftercare and notable facts
Recovery typically involves a hospital stay of several days and weeks to months of gradual return to normal activity. Cardiac rehabilitation, medications (antiplatelet agents, statins, blood pressure drugs) and lifestyle modification are central to preserving graft function. CABG is one of the most commonly performed major heart operations; it remains a key option when coronary artery disease is advanced or not amenable to percutaneous treatment. For general information about vascular sources used in the operation, see: blood vessels used for grafts. For an overview of patient information and preparation, consult: patient guidance on chest pain and treatment and surgical procedure overview.
Related articles
Author
AlegsaOnline.com Coronary artery bypass surgery (CABG) Leandro Alegsa
URL: https://en.alegsaonline.com/art/23186