Bronchopneumonia
Bronchopneumonia is an acute, patchy lung infection that begins in the bronchioles and spreads into adjacent air sacs. It most often follows bacterial infection and requires medical evaluation and antibiotic treatment.
Overview
Bronchopneumonia (also called bronchial or bronchogenic pneumonia) is an acute inflammatory condition that starts in the small airways and produces patchy areas of consolidation in the lung. The process begins in and around the bronchioles and extends into neighboring alveoli, often affecting multiple lobules rather than an entire lobe. It is one of the classical patterns of pneumonia described in clinical medicine.
Image gallery
3 Images

Causes and pathology
The driving problem is an infectious insult to airway and alveolar tissues, most commonly bacterial. Typical pathogens include streptococci, staphylococci, Haemophilus species and various gram-negative organisms; aspiration and hospital-acquired organisms are important in certain settings. Pathologically, bronchopneumonia shows neutrophil-rich exudates within bronchiolar walls and patchy alveolar filling with inflammatory material and fluid. This pattern contrasts with uniform consolidation of a whole lobe seen in lobar pneumonia.
Clinical features and diagnosis
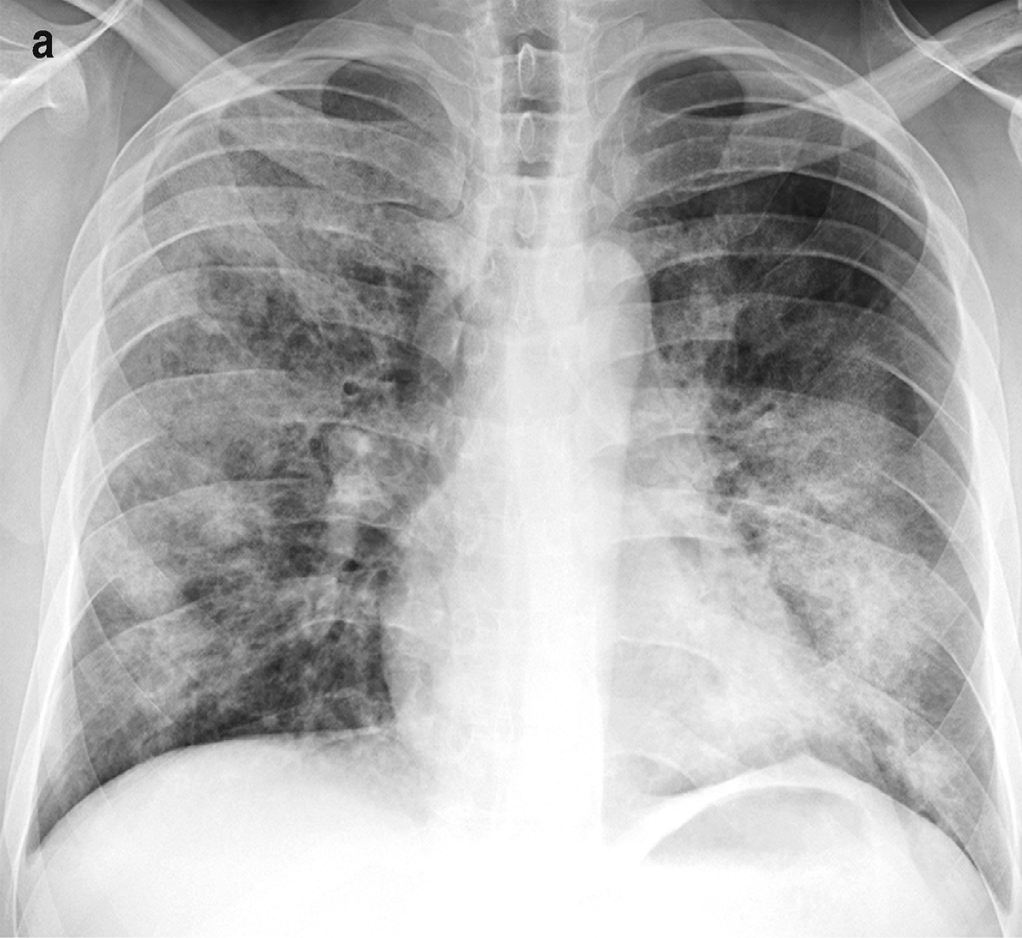
Symptoms can be similar to other lower respiratory infections and range from mild to severe: fever, cough with sputum production, shortness of breath, chest discomfort and rapid breathing. Signs on physical examination often include localized crackles and bronchial breath sounds over affected areas. Diagnosis relies on clinical assessment plus imaging and microbiology. Chest radiographs typically show multiple small, poorly defined opacities in one or both lungs; computed tomography provides greater detail. Laboratory testing may include blood counts, inflammation markers, sputum Gram stain and culture, and blood cultures when systemic infection is suspected.
Treatment and prevention
Management commonly begins with empiric antibiotics chosen to cover the likely organisms and is adjusted when culture results are available. Supportive measures include oxygen for hypoxaemia, fluids and ventilatory support in severe cases. Prevention focuses on reducing risk factors and vaccination: influenza and pneumococcal immunization, aspiration precautions, smoking cessation and infection control in healthcare settings can lower incidence and severity.
Complications, epidemiology and prognosis
Complications may include lung abscess, pleural effusion or empyema, respiratory failure and systemic sepsis, especially in elderly, very young or immunocompromised patients. Bronchopneumonia remains a common clinical pattern worldwide; advances in antibiotics, supportive care and vaccines have substantially improved outcomes compared with historical experience.
Distinctions and notable points
- Bronchopneumonia: multifocal, patchy consolidation originating in bronchioles and adjacent alveoli.
- Lobar pneumonia: homogeneous consolidation of an entire lobe, often due to a single organism.
- Bronchitis: inflammation principally of the bronchi without the alveolar consolidation that defines pneumonia.
For clinicians and patients, recognition of the pattern, prompt diagnosis and appropriate antimicrobial therapy are key to preventing complications. Further reading and clinical guidelines are available through standard medical resources and specialty societies (see clinical references).
Related articles
Author
AlegsaOnline.com Bronchopneumonia Leandro Alegsa
URL: https://en.alegsaonline.com/art/14671