Adrenoleukodystrophy (ALD): causes, symptoms, diagnosis and care
Adrenoleukodystrophy (ALD) is an X-linked disorder causing accumulation of very long‑chain fatty acids, progressive demyelination and adrenal failure. It mainly affects males; early diagnosis improves options.
Overview
Adrenoleukodystrophy (ALD) is a genetic disorder that primarily damages the nervous system and the adrenal glands. It is inherited in an X-linked pattern, so males are most often severely affected while females who carry the change in the responsible gene may develop milder symptoms later in life. The condition involves the abnormal build-up of very long‑chain fatty acids (VLCFAs) within cells, which contributes to inflammation and loss of the myelin sheath that insulates nerve fibers.
Image gallery
1 Image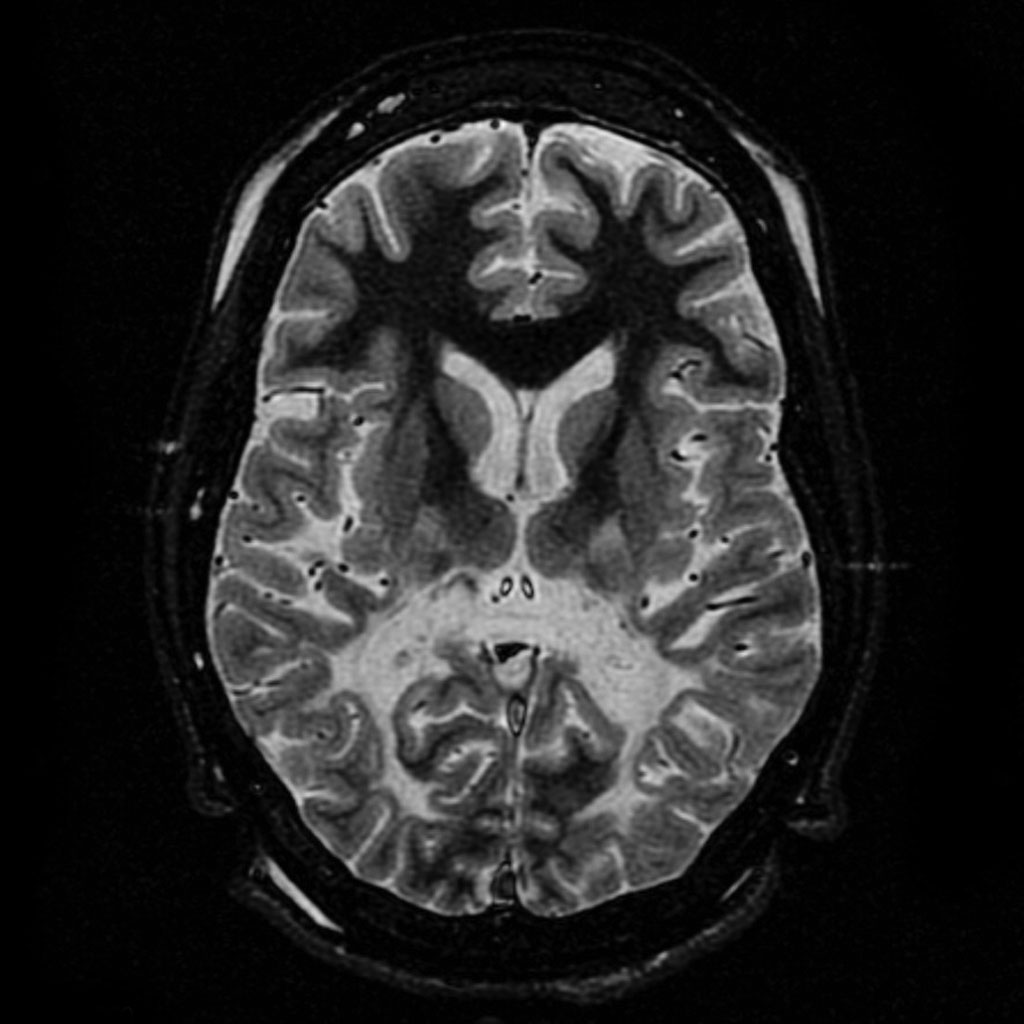
Causes and pathology
ALD most commonly results from mutations in a gene that encodes a peroxisomal membrane protein involved in transporting fatty acids into the peroxisome for degradation. When the transporter is defective, VLCFAs accumulate in the blood, brain, adrenal cortex and other tissues. The accumulation damages myelin (the insulating layer around nerves) and impairs adrenal function, producing a combination of neurological decline and endocrine insufficiency.
Clinical features and diagnosis
Clinical presentation is variable. The most dramatic form, childhood cerebral ALD, begins with behavioral changes and learning difficulties and can progress rapidly to loss of vision, hearing, coordination and seizures. An adult form, adrenomyeloneuropathy (AMN), causes progressive stiffness, weakness and sensory loss in the legs. Adrenal insufficiency (Addison disease) may precede or accompany neurologic symptoms.
- Common signs: behavioral change, school problems, gait disturbance, spasticity, vision or hearing loss.
- Diagnostic tools: measurement of VLCFAs in plasma, MRI of the brain showing demyelination patterns, and genetic testing to confirm mutations.
Treatment and prognosis
There is no universal cure, but several treatments can alter the course for selected patients. For boys with early cerebral involvement, hematopoietic stem cell transplantation can halt progression if done at an early stage. Hormone replacement is necessary for adrenal insufficiency. Dietary strategies and lipid‑lowering approaches (often discussed under names such as dietary supplements) have been used to modify VLCFA levels in asymptomatic individuals, though their ability to prevent cerebral disease is limited. Emerging options include gene therapy approaches and supportive measures to manage symptoms and improve quality of life.
- Interventions: adrenal steroid replacement, stem cell transplantation, symptomatic and rehabilitative care.
- Research directions: gene therapy, better biomarkers for early detection, improved neuroprotective strategies.
History, epidemiology and notable facts
ALD was recognized as a distinct condition in the 20th century and the underlying gene and biochemistry were elucidated as molecular techniques advanced. It is a rare disorder; estimates suggest it occurs in roughly one in every 17,000 births, though reported frequencies vary. Because early diagnosis changes treatment options and outcomes, newborn screening and family genetic testing are important in many regions.
Further resources
For patient information, scientific reviews and carrier guidance, consult reputable sources and genetic counseling services. The following links point to additional overviews, clinical guidelines and research summaries:
- General overview of ALD
- X-linked inheritance and implications
- Fatty acid metabolism and VLCFA biology
- Diagnostic testing approaches
- Genetic testing information
- Pathology of lipid accumulation
- Neurological manifestations and MRI findings
- Myelin disorders and differentiation
- Nerve and peripheral involvement
- Seizure management in leukodystrophies
- Behavioral and cognitive care strategies
- Speech and hearing support resources
- Current research and clinical trials
If ALD is suspected in an individual or family, prompt referral to a specialist in metabolic or genetic neurology and to a clinical genetics service is recommended to confirm the diagnosis, evaluate relatives and discuss treatment or surveillance options.
Related articles
Author
AlegsaOnline.com Adrenoleukodystrophy (ALD): causes, symptoms, diagnosis and care Leandro Alegsa
URL: https://en.alegsaonline.com/art/1067