Vitamin D — overview, function, sources, deficiency and safety
Vitamin D is a fat‑soluble secosteroid produced in skin with sunlight and obtained in diet or supplements. It supports calcium balance, bone health, immune function, and has distinct forms and public‑health uses.
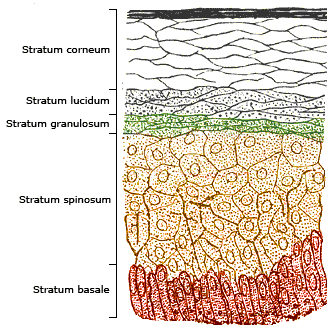
Overview: Vitamin D is a fat‑soluble nutrient that acts as a hormone in the body. It belongs to a family of secosteroids and is often described by clinicians as both a vitamin and an endocrinological regulator (hormone, steroid). The most important natural stimulus for its production is ultraviolet B (UVB) radiation from sunlight, which triggers chemical changes in the lower layers of the skin (sunlight, skin).
Image gallery
7 Images




Forms and metabolism
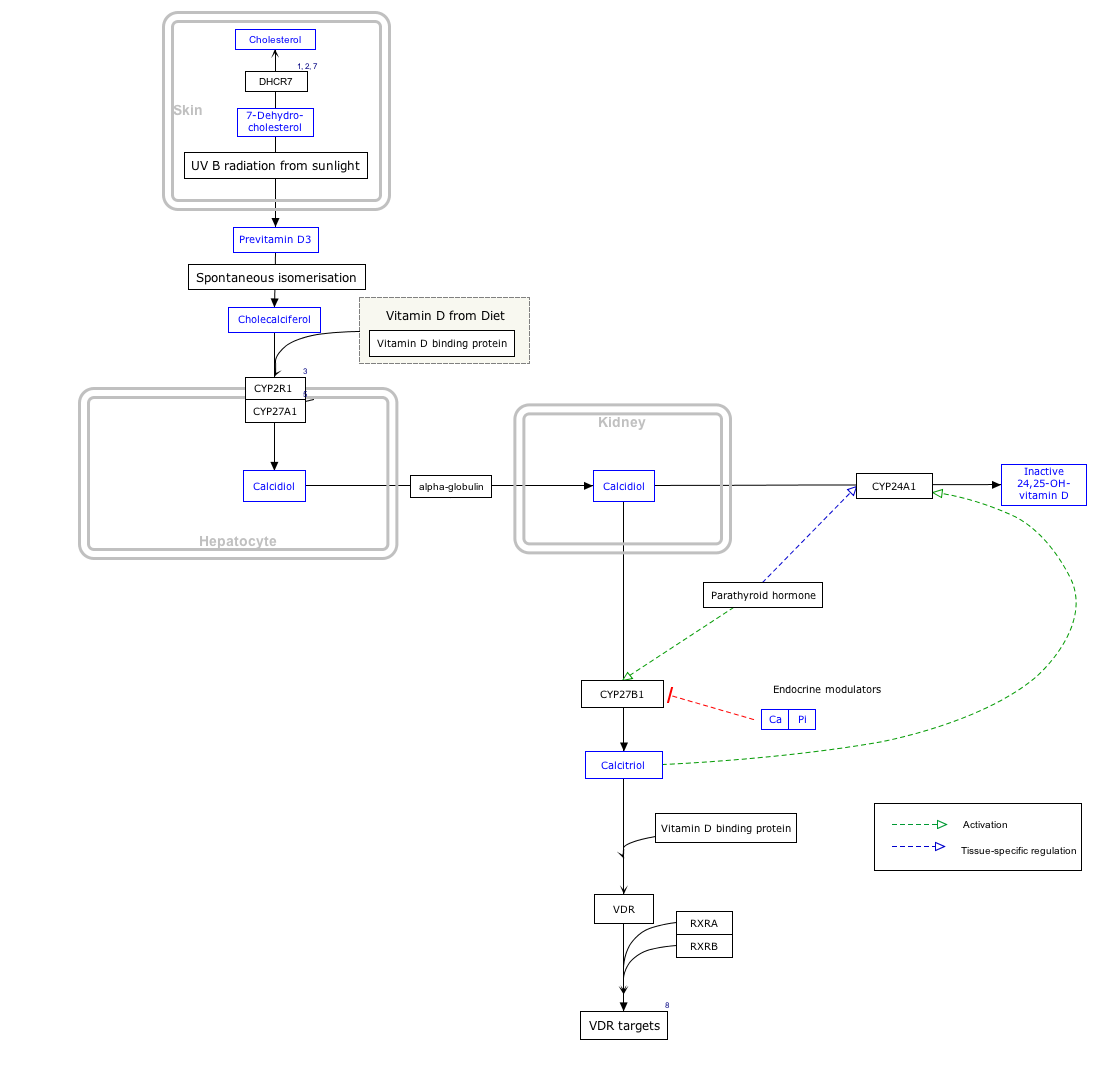
Two primary dietary forms exist: cholecalciferol (vitamin D3) and ergocalciferol (vitamin D2). Both are converted in the liver and kidney into an active hormone (calcitriol) that binds receptors in bone, intestine, kidney and other tissues. The active hormone helps regulate absorption and distribution of calcium and phosphate, which are critical for healthy bones and muscles.
Sources and public‑health measures
Natural food sources are limited but include fatty fish, egg yolks and certain mushrooms. Many countries mandate or encourage fortification of staple foods such as milk and plant milks (fortified milk) to reduce deficiency. Over‑the‑counter supplements are widely available (supplements), and public guidance often recommends supplementation for groups at risk of low levels.
- Sunlight: UVB exposure enables skin production but varies with season, latitude and skin pigment.
- Diet and fortification: Fish, fortified foods, and supplements are the main sources when sunlight is insufficient.
- Storage: Being a fat‑soluble compound, excess vitamin D is stored in body fat (adipose tissue) and released over time.
Health roles and clinical aspects
Vitamin D is best known for supporting skeletal health by promoting intestinal calcium uptake and maintaining serum calcium and phosphate. It also influences muscle function and has modulatory effects on the immune system. Populations at higher risk of low vitamin D include people with limited sun exposure, darker skin, older adults, those with malabsorption, and individuals living at high latitudes.
Deficiency can cause rickets in children and osteomalacia in adults, conditions characterized by impaired bone mineralization. Mild deficiency is associated with reduced bone strength and higher fracture risk. Excess is uncommon from sun exposure but can occur with very high supplemental intakes and may lead to hypercalcemia and related symptoms; therefore supplementation is guided by clinical context and measured blood levels.
Distinctions and practical guidance
Clinically, vitamin D status is assessed by measuring circulating 25‑hydroxyvitamin D. Differences between D2 and D3, seasonal variation, body fat, age and some medications affect levels and response to supplements. Public‑health strategies—screening in high‑risk groups, targeted supplementation and food fortification—aim to balance preventing deficiency while avoiding unnecessary high dosing. For authoritative guidance, consult local health recommendations or clinical references (more, supplements).
Related articles
Author
AlegsaOnline.com Vitamin D — overview, function, sources, deficiency and safety Leandro Alegsa
URL: https://en.alegsaonline.com/art/105653
Sources
- iom.edu : iom.edu
- ncbi.nlm.nih.gov : "Estimates of optimal vitamin D status"
- doi.org : 10.1007/s00198-005-1867-7
- pubmed.ncbi.nlm.nih.gov : 15776217