Basilar-type migraine (migraine with brainstem aura)
A migraine variant characterized by brainstem and posterior fossa symptoms that often precede headache. Covers presentation, likely mechanisms, diagnosis, and management considerations.
Basilar-type migraine is a clinical migraine variant in which transient symptoms of the brainstem and posterior fossa appear before or during the headache phase. In contemporary headache classification it is usually referred to as "migraine with brainstem aura"; the older name persists in many clinical descriptions. The condition most often begins in adolescence or young adulthood and is typically seen in people who also experience more common forms of migraine with aura. Migraine and aura terminology appear frequently in discussions of this syndrome.
Image gallery
2 Images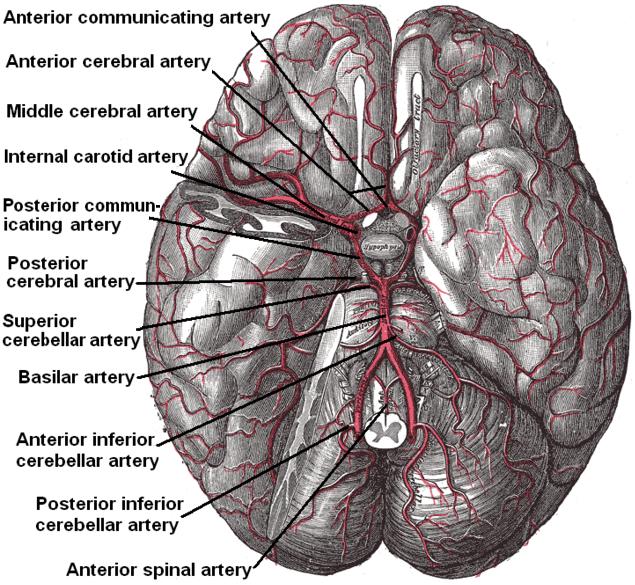

Typical features and symptoms
Symptoms attributed to basilar-type migraine arise from dysfunction in structures of the posterior fossa, including the brainstem, occipital cortex and cerebellum. Patients commonly report visual disturbance and other brainstem-related phenomena which may include:
- Vertigo or dizziness
- Tinnitus or altered hearing
- Diplopia (double vision) and other visual changes often starting in the occipital region
- Dysarthria or slurred speech
- Ataxia or unsteadiness related to cerebellar involvement
- Decreased level of consciousness or profound confusion in some attacks
These transient neurological signs usually precede the painful headache phase, which often begins in the lower posterior part of the head. The pain may be bilateral and range from moderate to severe. Importantly, pure basilar-type or brainstem aura does not typically include persistent motor weakness; if hemiparesis or prolonged motor deficit is present, other migraine subtypes or alternative diagnoses should be considered.
Pathophysiology and terminology
The exact cause is not settled. A leading hypothesis links migraine aura to cortical spreading depression and to transient dysfunction of brainstem networks that modulate sensory processing and vascular tone. Early descriptions named the disorder for the basilar artery because many affected regions receive circulation from that vessel, but subsequent research did not confirm a necessary role for basilar artery ischemia. In modern classification the phrase "brainstem aura" emphasizes the clinical syndrome rather than an assumed vascular culprit. References to anatomical terms such as skull base or the basilar artery reflect historical etymology rather than definitive mechanism.
Diagnosis and important distinctions
Diagnosis rests on clinical history and neurological examination supported by criteria from headache classification systems. Because symptoms overlap with acute posterior circulation ischemia, demyelinating disease, seizures, and other brainstem disorders, clinicians often use imaging (magnetic resonance imaging) and other tests to exclude structural or vascular causes. Standard tests such as electroencephalography are not diagnostic for basilar-type migraine. When motor weakness accompanies aura, consider other headache syndromes such as hemiplegic migraine and seek urgent evaluation.
Management and prognosis
Treatment aligns with general migraine care: acute symptom control (analgesics, antiemetics) and preventive strategies when attacks are frequent or disabling. Some specific acute agents have been used with caution because of theoretical vascular effects; discuss triptans and other prescription options with a clinician familiar with the individual patient. Preventive approaches include lifestyle modification, trigger avoidance, and medications chosen for the patient’s overall health and comorbidities. Most people with basilar-type migraine experience improvement over time, though attacks can recur periodically.
Clinical importance and further reading
Basilar-type migraine is notable for its brainstem and posterior fossa symptom cluster and for the need to distinguish benign migraine aura from potentially life‑threatening conditions such as stroke. Because diagnostic and treatment choices may vary by region and guideline, professional sources and headache specialists can provide tailored advice. For background on related topics see brain anatomy, brainstem function, and vascular supply distribution. Additional references and patient resources are available from clinical headache organizations and specialty guidelines. Aura descriptions and general migraine management appear in many review articles and guideline statements; consult trusted clinical material for current recommendations. Occipital symptom patterns and cerebellar signs warrant careful evaluation. For international classification details see resources linked by professional headache bodies and local neurology services. Skull base anatomy and basilar circulation are useful for understanding the historical naming of the disorder.
Related articles
Author
AlegsaOnline.com Basilar-type migraine (migraine with brainstem aura) Leandro Alegsa
URL: https://en.alegsaonline.com/art/9243
Sources
- merriam-webster.com : basilar