Optic nerve (cranial nerve II)
The optic nerve transmits visual signals from retinal ganglion cells to central visual centers. It is developmentally and structurally part of the central nervous system and essential for sight and visual fields.
Overview
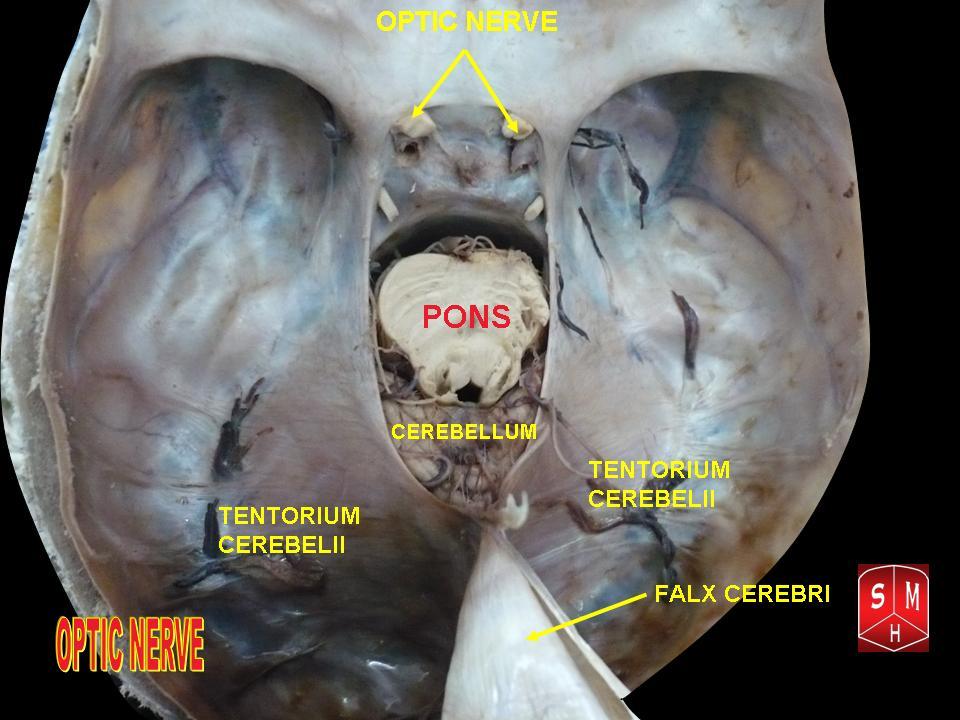
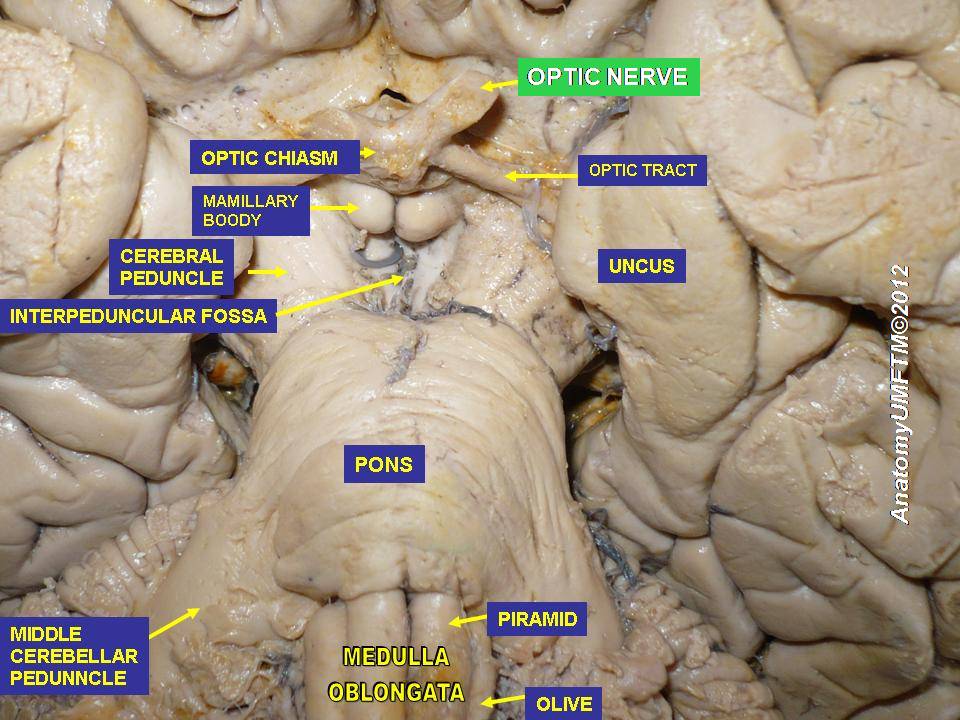
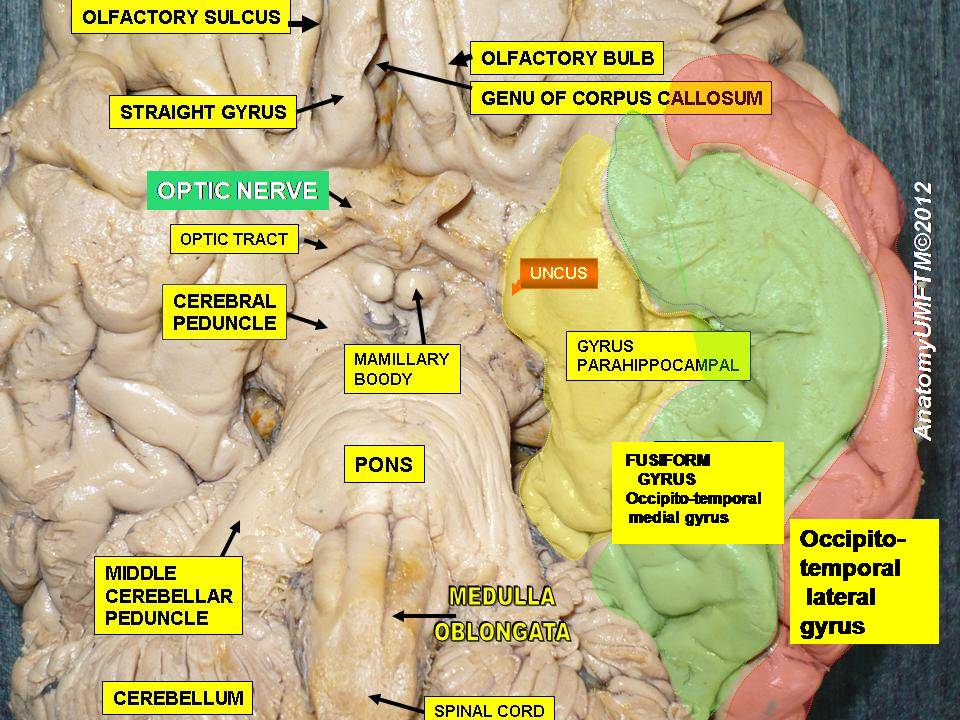
The optic nerve, or cranial nerve II, conveys visual information from the retina to the brain. Although described as a cranial nerve, it is anatomically and developmentally continuous with the central nervous system, being myelinated by oligodendrocytes and enclosed by the meninges. Axons of retinal ganglion cells bundle at the optic disc and leave the eye as the optic nerve proper.
Image gallery
10 Images





Structure and pathway
Each optic nerve courses posteriorly from the globe, meets its counterpart at the optic chiasm where some fibers cross, and continues as optic tracts to subcortical targets. The principal relay for conscious vision is the lateral geniculate nucleus, whose neurons project to the visual cortex. Other important projections include the pretectal area for pupillary reflexes and the suprachiasmatic nucleus for circadian regulation.
Function and signal processing
The optic nerve transmits spatial, contrast and temporal information encoded by photoreceptors and processed by retinal interneurons. The light image on the retina is inverted and reversed relative to external space; higher visual pathways interpret these patterns so perception corresponds to the correct orientation and location. Visual signals carried by the optic nerve support perception, reflexes and eye movement coordination.
Origins, development and classification
Embryologically the optic nerve develops as an outgrowth of the forebrain, which explains its CNS-like features despite being numbered among the cranial nerves. Because its supporting cells and coverings are characteristic of central nervous tissue, clinicians often manage optic nerve disorders with neuroimaging and treatments directed at CNS processes. For context about cranial nerve numbering and relationships, see material on cranial nerves.
Blood supply and metabolism
The optic nerve head and anterior nerve receive blood from small branches of the ophthalmic and posterior ciliary circulations; more posterior segments are supplied by pial vessels. The nerve's high metabolic demands make it vulnerable to ischemia, inflammation and pressure-related injury.
Clinical significance
Lesions of the optic nerve cause characteristic visual field defects depending on location: defects in one eye with anterior lesions, bitemporal field loss with chiasmal compression, and homonymous defects with postchiasmal lesions. Common conditions include optic neuritis, glaucomatous optic neuropathy, ischemic optic neuropathy, compressive lesions, traumatic injury and swelling from raised intracranial pressure (papilledema).
- Typical signs: reduced visual acuity, color vision loss, afferent pupillary defect, visual field defects.
- Common investigations: visual field testing (perimetry), fundoscopic exam, optical coherence tomography (OCT), and neuroimaging such as MRI.
Diagnosis and management
Evaluation aims to localize the lesion and detect reversible causes. Management depends on cause: inflammatory optic neuritis may be treated with corticosteroids in selected situations; compressive lesions are managed by surgery or radiotherapy when appropriate; glaucoma care focuses on lowering intraocular pressure. Imaging of the brain and orbits is often used to assess anatomy and exclude mass lesions.
Research, prognosis and prevention
Prognosis varies with cause and promptness of treatment. Research continues into neuroprotection, remyelination and regenerative strategies to preserve or restore optic nerve function. Preventive measures for some causes include vascular risk factor control and regular ophthalmic screening for glaucoma.
Further reading
For general anatomy and clinical context, consult resources on the central nervous system, the eye, and the retina. Overviews of cranial nerve function and neuro-ophthalmology may be found under topics covering cranial nerves and visual pathways; introductory material about brain structure and function is available in broader texts about the brain.
Related articles
Author
AlegsaOnline.com Optic nerve (cranial nerve II) Leandro Alegsa
URL: https://en.alegsaonline.com/art/72882