Multiple myeloma: overview, diagnosis, treatment, and key facts
Multiple myeloma is a cancer of plasma cells that affects bone, kidney and immunity. This article explains features, diagnosis, common treatments, supportive care, and related conditions.

Multiple myeloma is a malignant disorder of plasma cells — the antibody-producing white blood cells in bone marrow. It is often described as a form of blood cancer that produces a characteristic monoclonal protein. For a general context see cancer information. Myeloma typically develops over time and may follow precursor stages such as monoclonal gammopathy of undetermined significance (MGUS) or smoldering myeloma.
Image gallery
10 Images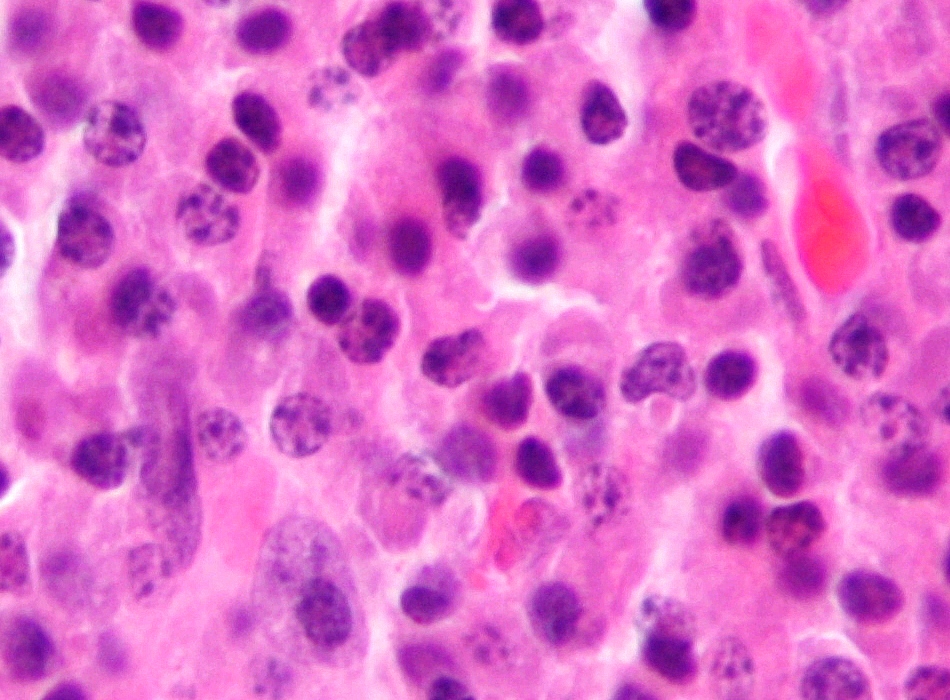









Clinical features and complications
Symptoms can be varied and sometimes subtle. Common problems include bone pain, anemia, recurrent infections and kidney dysfunction. The classic mnemonic CRAB summarizes key complications: hyperCalcemia, Renal impairment, Anemia and Bone lesions. For an outline of presenting symptoms see symptoms and signs.
Diagnosis and evaluation
Diagnosis relies on laboratory and imaging studies plus bone marrow examination. Typical tests include serum and urine protein electrophoresis and immunofixation to detect an abnormal M-protein, serum free light-chain assays, complete blood count and metabolic panel, and bone marrow biopsy showing clonal plasma cells. Imaging (skeletal survey, MRI or PET) assesses lytic bone lesions.
Treatment approaches
Management combines disease-directed therapy and supportive care. Chemotherapy and targeted agents reduce malignant plasma cells; historically regimens such as vincristine, doxorubicin and dexamethasone were used, and modern combinations often include proteasome inhibitors and immunomodulatory drugs. For general chemotherapy information see chemotherapy overview. Common drugs include thalidomide, bortezomib (Velcade), and alkylators such as melphalan. High-dose therapy with autologous stem cell transplantation is an option for suitable patients.
Supportive care and newer therapies
Supportive measures aim to prevent fractures, reduce bone pain and limit infections and renal injury. Bisphosphonates, analgesia, antibiotics, vaccinations and careful hydration are frequently used. Recent advances include monoclonal antibodies, novel small molecules and cellular therapies under study; these have broadened options for patients with relapsed or refractory disease.
Prognosis and related conditions
Prognosis varies with disease stage, biology and treatment access. Early-stage precursor states such as MGUS require monitoring because they may never progress. Because management and outcomes evolve rapidly, patients are usually followed by specialists and offered clinical trials when appropriate.
- Key signs: bone pain, anemia, kidney problems, infections.
- Essential tests: serum/urine protein studies, bone marrow biopsy, imaging.
- Therapies: combinations of chemotherapy, immunomodulators, proteasome inhibitors, steroids, and supportive care; transplantation in eligible patients.
For more detailed and individualized guidance patients should consult hematology specialists and reliable medical resources or clinical guidelines provided by professional organizations.
Related articles
Author
AlegsaOnline.com Multiple myeloma: overview, diagnosis, treatment, and key facts Leandro Alegsa
URL: https://en.alegsaonline.com/art/67476