Multiple sclerosis — autoimmune demyelinating disease of the central nervous system
Multiple sclerosis (MS) is a chronic neurological disorder in which the immune system damages myelin in the central nervous system, producing variable neurological symptoms and a course that ranges from relapsing to progressive.
Multiple sclerosis (MS) is a chronic disorder of the central nervous system (CNS) in which immune-related processes damage myelin, the insulating layer that surrounds nerve fibers. The consequence is impaired electrical conduction in the brain, spinal cord and optic nerves, producing symptoms that can include visual disturbance, limb weakness, sensory changes, imbalance, fatigue and cognitive difficulties. Presentation, pace and severity differ widely from person to person.
Image gallery
10 Images







Key characteristics
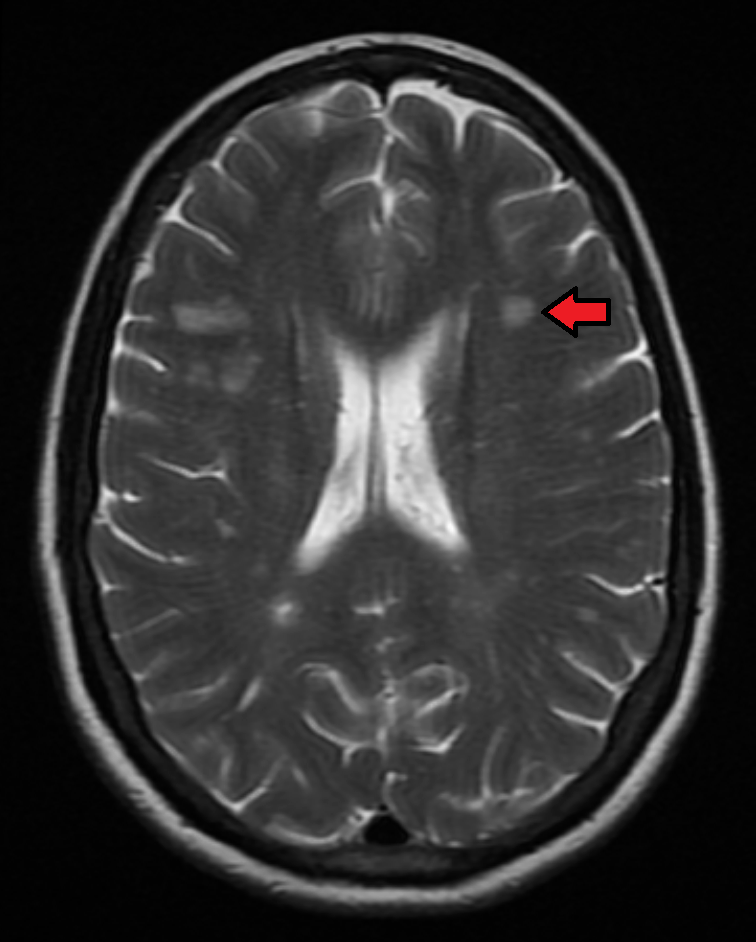
MS is defined by inflammatory demyelination and neurodegeneration within the CNS. Lesions — areas of myelin loss and axonal injury — may be visible on magnetic resonance imaging (MRI) and are often scattered in space and time. Typical hallmarks include relapses (episodes of new or worsening neurological dysfunction) and varying degrees of recovery. Over time some people develop a steady accumulation of disability.
Common symptoms and clinical types
- Symptoms: visual problems (optic neuritis), weakness, numbness, spasticity, coordination and balance problems, bladder or bowel dysfunction, fatigue, pain and cognitive changes.
- Clinical courses: relapsing–remitting MS (most common at onset), secondary progressive MS (gradual worsening after an initial relapsing course), and primary progressive MS (steady progression from onset).
Causes and risk factors
The exact cause of MS remains unknown. It is generally regarded as an immune-mediated disease influenced by genetic susceptibility and environmental factors. Risk factors that are widely recognized include a family history of MS, female sex, lower vitamin D status and prior infection with certain viruses. Research indicates that aberrant immune responses target myelin-producing cells (oligodendrocytes) in the CNS, but precise triggers and mechanisms are under active study.
Diagnosis and investigation
Diagnosis is clinical and supported by tests showing lesions separated in space and time. MRI of the brain and spinal cord is the principal imaging tool to detect typical demyelinating plaques. Additional investigations may include lumbar puncture to detect inflammatory markers in cerebrospinal fluid, and evoked potentials to document slowed nerve conduction. Specialist neurological assessment integrates history, examination and investigation results to reach a diagnosis.
Treatment and management
Management has two complementary aims: altering the disease course and treating symptoms. Disease-modifying therapies (DMTs) reduce relapse frequency and slow progression for many people; these include injectable agents, oral medications and monoclonal antibodies. Acute relapses are often treated with short courses of corticosteroids. Supportive care addresses spasticity, pain, bladder dysfunction, mobility and fatigue, and rehabilitation (physiotherapy, occupational therapy, cognitive support) plays a central role in maintaining function and quality of life.
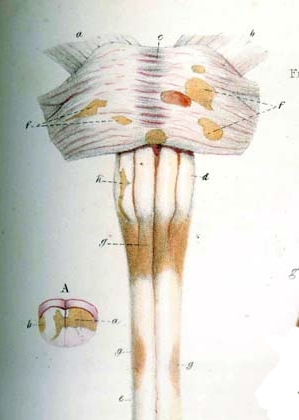
History, prognosis and public health
Multiple sclerosis was first described in detail in the 19th century and remains a major cause of neurological disability in young adults in many regions. Prognosis is variable: some people experience mild, intermittent symptoms for decades, while others accumulate disability more rapidly. Advances in imaging and therapy over recent decades have improved diagnostic accuracy and outcomes for many. For up-to-date overviews and clinical guidance, readers can consult authoritative resources such as disease summaries, immunology references at immune system resources, basic information on myelin at myelin-focused pages, and central nervous system overviews at CNS information.
Notable facts: MS is more common in temperate climates and typically begins in early adulthood. Research remains active on causes, biomarkers, neuroprotection and strategies for repair of myelin and axons. Early diagnosis and individualized therapy can substantially affect long-term outcomes.
Questions and answers
Q: What is multiple sclerosis?
A: Multiple sclerosis (MS) is a serious health condition where the body's natural immune system damages the fatty coverings called myelin sheaths around nerve cells in the central nervous system.
Q: How does MS affect the body?
A: MS can cause different effects in different people, including poor body function, eyesight, speech, and mind function.
Q: Does MS affect people's life expectancy?
A: Yes, people with MS do not normally live as long as healthy people.
Q: What is the role of myelin sheaths in healthy people?
A: Myelin sheaths help neurons work properly by keeping electric signals moving quickly through long, narrow axons.
Q: What happens to myelin sheaths in people with MS?
A: In people with MS, immune cells cause inflammation within the central nervous system and result in the loss of the protective insulator called demyelination.
Q: How does the loss of myelin sheaths impair the body's ability to regrow its myelin?
A: Progressive loss of the myelin sheath and myelin-producing cells impair the body's ability to regrow its myelin.
Q: Why does the loss of myelin sheaths cause problems with the mind and body?
A: Without the protective covering, the signals between neurons do not travel well, and the mind and body cannot function normally.
Related articles
Author
AlegsaOnline.com Multiple sclerosis — autoimmune demyelinating disease of the central nervous system Leandro Alegsa
URL: https://en.alegsaonline.com/art/67479
Sources
- pubmed.ncbi.nlm.nih.gov : 18970977
- pubmed.ncbi.nlm.nih.gov : 11955556
- pubmed.ncbi.nlm.nih.gov : 14747002
- pubmed.ncbi.nlm.nih.gov : 15556803
- pubmed.ncbi.nlm.nih.gov : 17492755
- pubmed.ncbi.nlm.nih.gov : 20494325
- pubmed.ncbi.nlm.nih.gov : 17444504
- pubmed.ncbi.nlm.nih.gov : 8269393
- pubmed.ncbi.nlm.nih.gov : 15721830
- pubmed.ncbi.nlm.nih.gov : 8780061
- doi.org : 10.1093/brain/awq250
- pubmed.ncbi.nlm.nih.gov : 17351524
- pubmed.ncbi.nlm.nih.gov : 18606967
- pubmed.ncbi.nlm.nih.gov : 11456302
- pubmed.ncbi.nlm.nih.gov : 16945427