Glioblastoma multiforme: overview, pathology, diagnosis, and management
Aggressive WHO grade IV primary brain tumor marked by rapid growth, infiltration, and necrosis. Covers symptoms, imaging and histology, molecular markers, treatment options, prognosis, and research directions.
Overview
Glioblastoma multiforme (commonly abbreviated GBM) is the most aggressive primary malignant brain tumor in adults. Classified as a World Health Organization (WHO) grade IV astrocytic tumor, GBM grows rapidly and invades surrounding brain tissue, making complete surgical removal difficult. The disease typically presents with neurological deficits, headaches, seizures, or changes in cognition depending on tumor location.
Image gallery
9 Images






Key characteristics
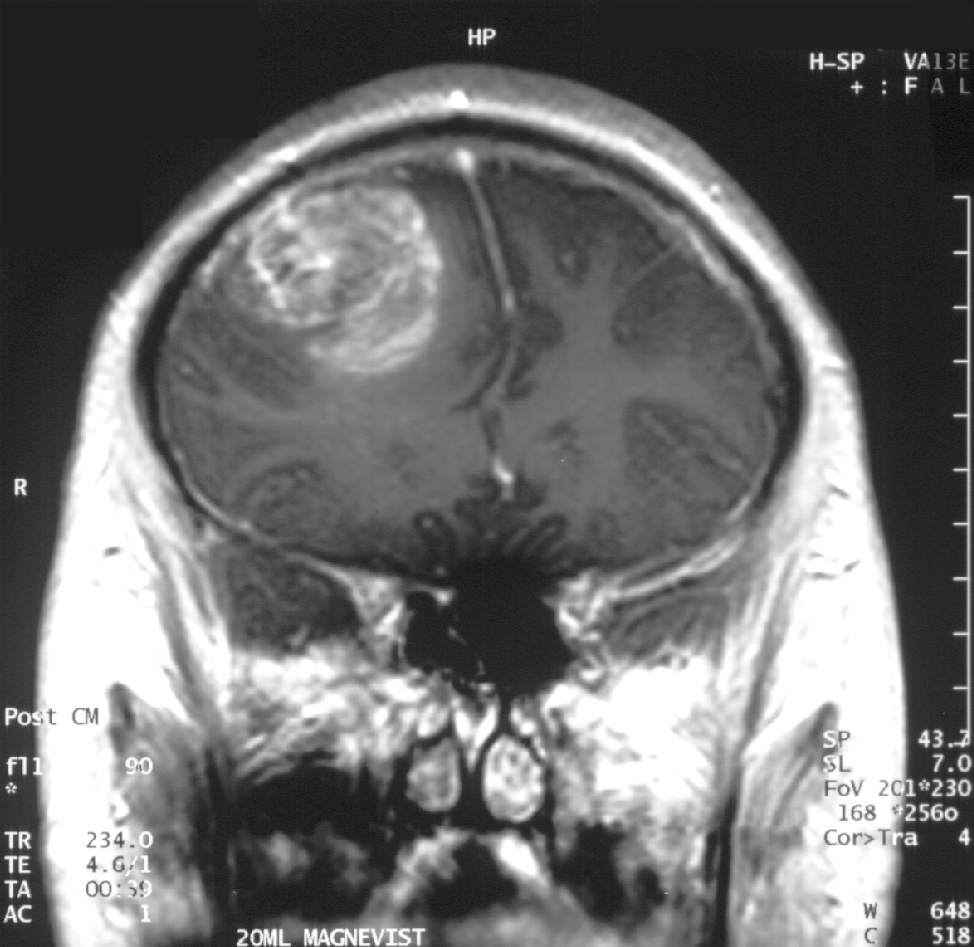
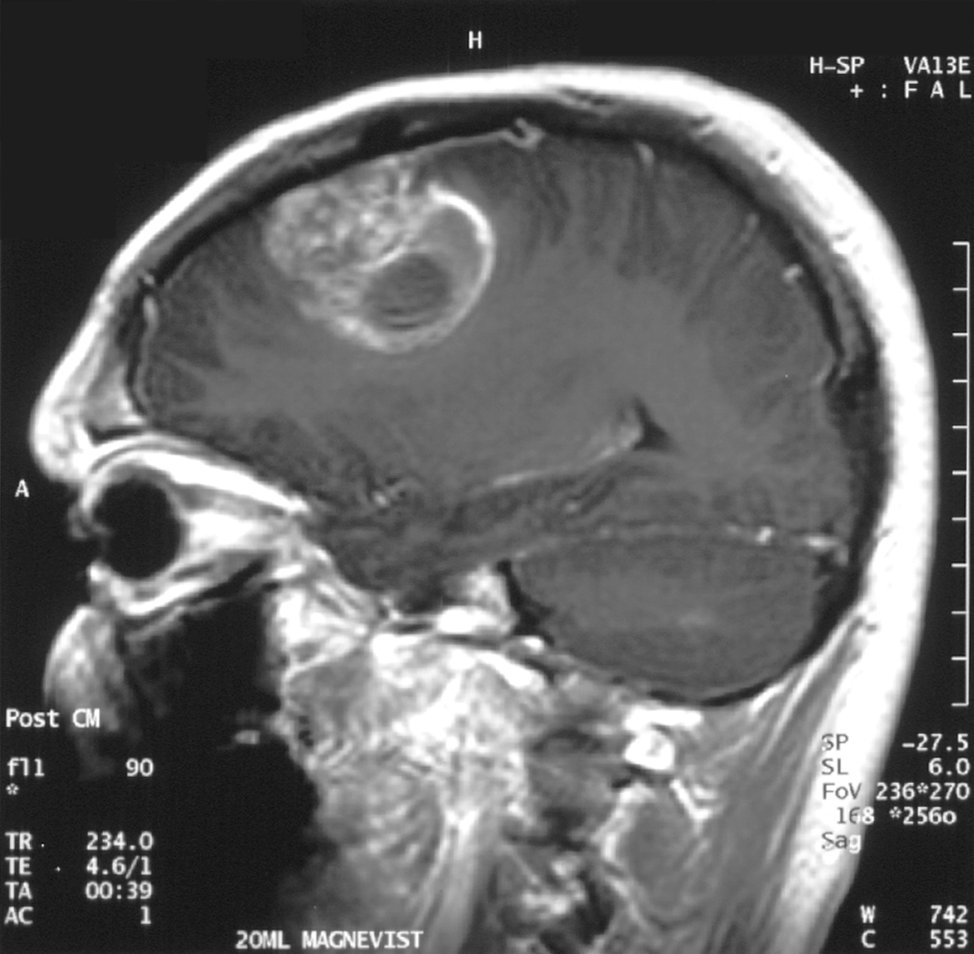
Histologically GBM is notable for marked cellular atypia, brisk mitotic activity, areas of necrosis, and microvascular proliferation. On magnetic resonance imaging (MRI) it often appears as a heterogeneous, ring-enhancing mass with surrounding edema. At the molecular level, GBM is heterogeneous: many tumors are IDH-wildtype and harbor alterations such as EGFR amplification, while a subset arises from lower-grade gliomas and shows IDH mutations.
Presentation and diagnosis
- Common symptoms: progressive focal neurological signs, persistent headaches, and seizures.
- Primary diagnostic tools: MRI with contrast, followed by histological confirmation via biopsy or resection.
- Important biomarkers: IDH mutation status and MGMT promoter methylation, which help guide prognosis and treatment planning.
Treatment and prognosis
Standard management combines maximal safe surgical resection with radiotherapy and concurrent and adjuvant alkylating chemotherapy (temozolomide). Additional modalities such as tumor-treating fields and clinical trials for targeted therapies or immunotherapy may be considered. Despite treatment, recurrence is common and overall outlook remains poor; survival is typically measured in months to a few years, and outcomes vary with age, functional status, and molecular markers. For information about prognosis and support, see resources discussing outcomes.
Research and notable facts
Research focuses on understanding tumor heterogeneity, overcoming the blood–brain barrier, and finding effective targeted or immune-based therapies. MGMT promoter methylation predicts better response to alkylating agents, and IDH-mutant tumors usually have a different clinical course than IDH-wildtype tumors. Multidisciplinary care including neurosurgery, neuro-oncology, radiation oncology, neuropathology, and palliative services is essential for optimal management.
Related articles
Author
AlegsaOnline.com Glioblastoma multiforme: overview, pathology, diagnosis, and management Leandro Alegsa
URL: https://en.alegsaonline.com/art/39211