Endometrial cancer: causes, diagnosis, treatment, and prognosis
A clear, concise overview of endometrial cancer — tumour of the uterine lining — covering causes, symptoms, diagnosis, staging, treatment options, prevention and noteworthy distinctions.
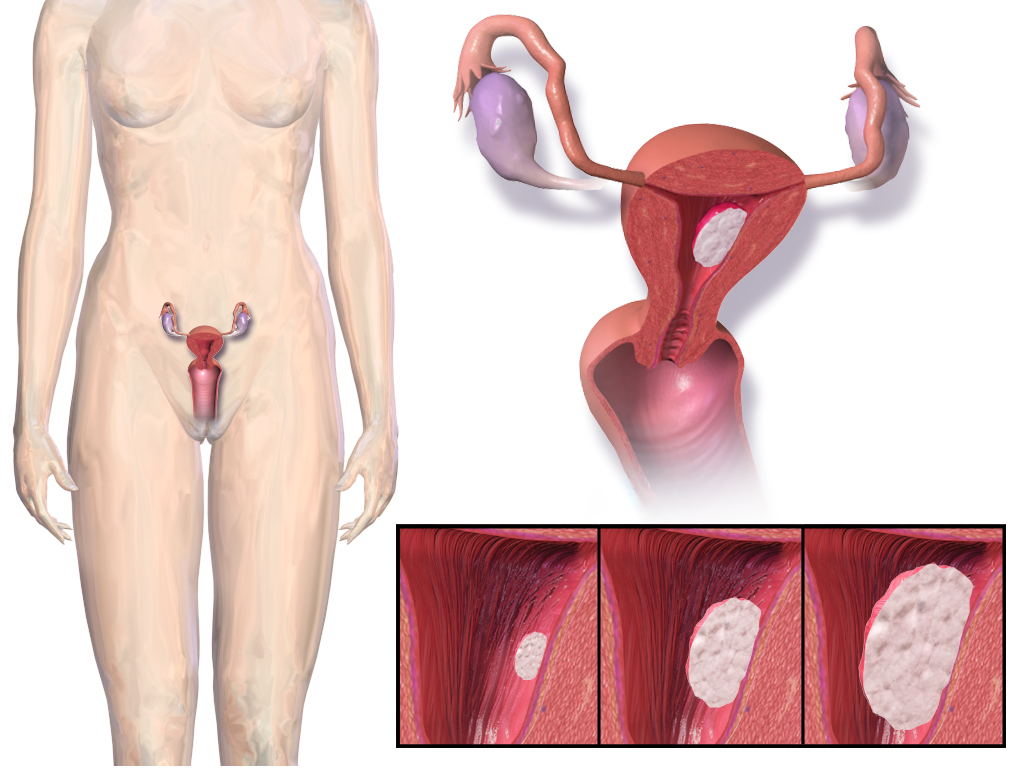
Overview: Endometrial cancer arises from the cells of the endometrium, the inner lining of the uterus. It is the most common gynecologic malignancy in many countries and is often identified at an early stage because it frequently produces symptoms such as abnormal vaginal bleeding. Early detection typically leads to better outcomes than for many other cancers.
Image gallery
10 Images







Biology and types
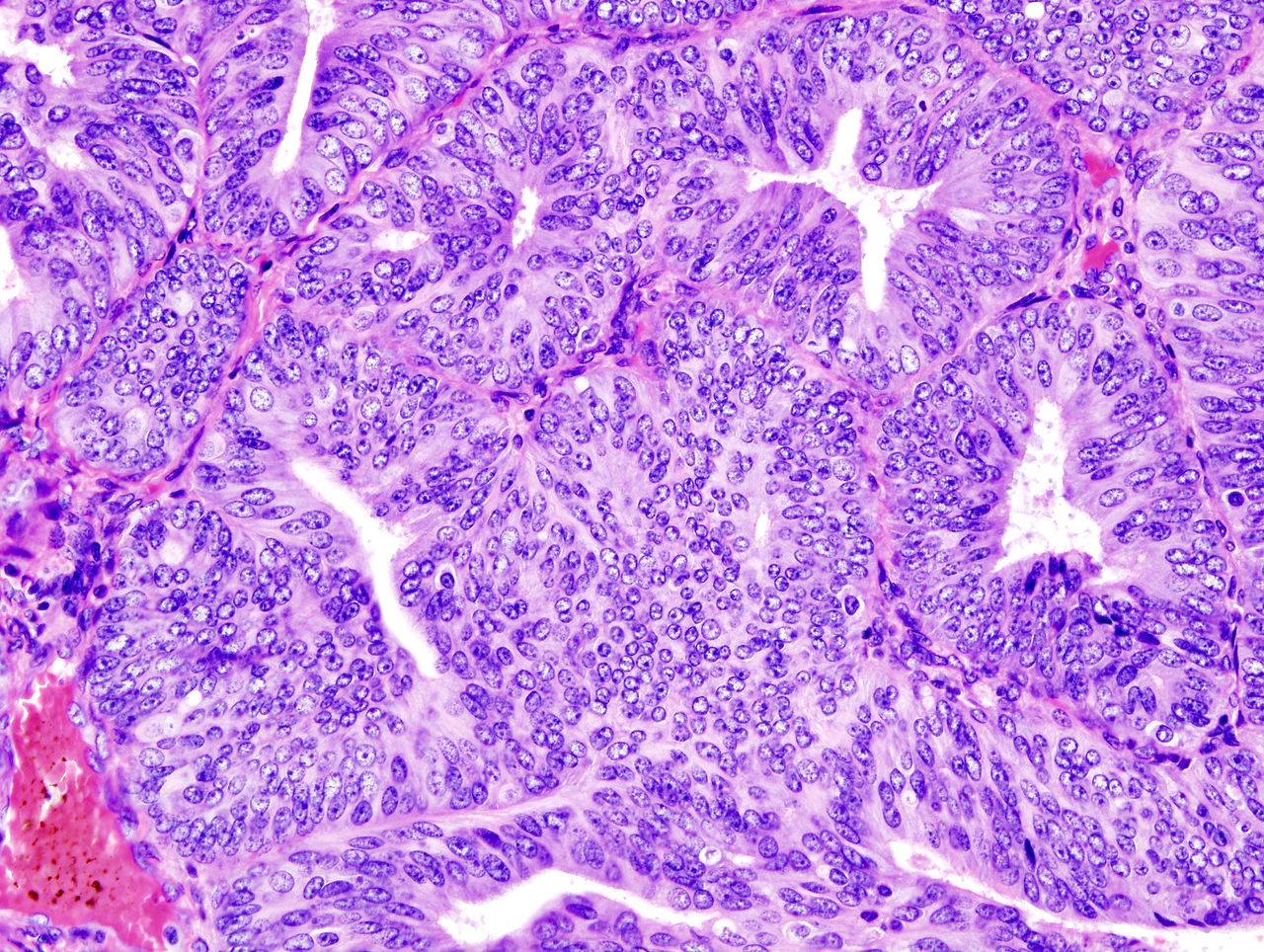
Most cases begin as malignant growths of glandular endometrial cells. Pathologists classify tumours into several histologic types with distinct behavior. The common form, often called endometrioid carcinoma, is typically associated with hormonal risk factors and generally has a more favorable prognosis. Less common types—such as serous or clear-cell carcinomas—tend to be more aggressive and may require different treatment approaches. Modern molecular profiling (including tests for mismatch repair defects, POLE mutations and p53 abnormalities) is increasingly used to refine prognosis and guide therapy.
Risk factors and symptoms
- Typical risk factors: increasing age after menopause, obesity, prolonged exposure to estrogen unopposed by progesterone, certain hormonal medications, and some reproductive histories.
- Other contributors can include diabetes, polycystic ovary syndrome and a family history of related cancers.
- Common symptoms: abnormal uterine bleeding (especially after menopause), pelvic pain or a palpable mass in more advanced disease.
Diagnosis and staging
Initial assessment often includes a clinical exam and imaging such as transvaginal ultrasound. Definitive diagnosis requires sampling of the endometrium, typically by office endometrial biopsy or dilation and curettage; hysteroscopy may aid evaluation. Staging systems—commonly based on surgical findings—describe tumour extent within the uterus, cervix, adnexa, lymph nodes and distant sites, and help determine prognosis and treatment plans.
Treatment and follow-up
Primary treatment for most localized cases is surgery, usually total hysterectomy with removal of both ovaries and fallopian tubes in many patients. Depending on stage, grade and molecular features, additional therapies can include radiation, chemotherapy or hormonal agents (for hormone-sensitive disease). Advanced or recurrent disease may be managed with systemic therapies or clinical trials of targeted agents. Long-term follow-up typically addresses surveillance for recurrence and management of treatment effects.
Prevention, screening and notable facts
- There is no recommended routine screening for average-risk women; vigilance for abnormal bleeding is important.
- Risk reduction strategies include managing obesity, careful use of hormone therapy, and, for some women at high genetic risk, preventive surgical options.
- Research continues into molecular classification and targeted treatments to personalize care and improve outcomes.
For more detailed clinical guidelines and patient information, consult specialty resources or professional societies: overview resources, information about the endometrium, and educational material about the uterus.
Related articles
Author
AlegsaOnline.com Endometrial cancer: causes, diagnosis, treatment, and prognosis Leandro Alegsa
URL: https://en.alegsaonline.com/art/31387