Yellow fever: cause, transmission, prevention, and historical impact
Yellow fever is an acute mosquito‑transmitted viral disease that can cause fever, jaundice and hemorrhage; it is preventable by a live vaccine and controlled by vaccination and vector control.
Overview
Yellow fever is an acute viral disease caused by the yellow fever virus, a member of the Flavivirus genus. Clinical presentation ranges from a self-limited febrile illness to a severe toxic form with jaundice (yellowing of the skin and eyes), bleeding and organ dysfunction. The name of the disease refers to the jaundice that develops in some severe cases; for information on jaundice see jaundice. The disease remains a public-health concern in parts of tropical Africa and South America.
Image gallery
10 Images








Cause and virology
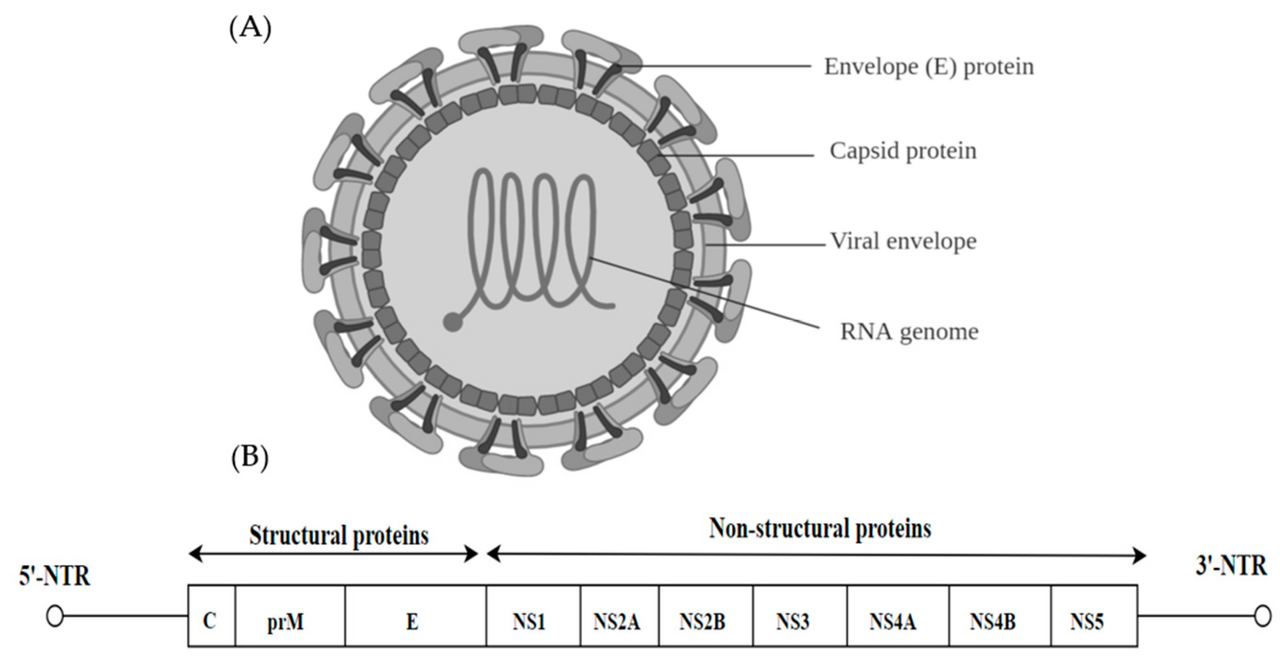
The agent is a single‑stranded RNA virus transmitted between vertebrate hosts and mosquitoes. The virus replicates in the skin and bloodstream and can affect the liver, which explains the characteristic jaundice. Understanding of the virus’s biology has supported vaccine development and public-health strategies.
Clinical features and diagnosis
After an incubation period of about 3–6 days, typical early symptoms include fever, headache, muscle pain, nausea and vomiting. Many patients recover after this initial phase. A smaller proportion progress to a severe phase with high fever, jaundice, dark urine and bleeding from the mouth, nose or gastrointestinal tract. Laboratory diagnosis uses detection of virus-specific antibodies, antigen, or viral RNA and assessment of liver enzymes. Treatment is supportive; there is no widely available specific antiviral therapy.
Transmission and vectors
The virus is transmitted to humans by infected female mosquitoes. The principal urban vector is Aedes aegypti, which thrives in and around human habitation. In forested areas, sylvatic cycles involve nonhuman primates and forest mosquitoes such as Haemagogus and Sabethes; people entering these areas can be infected and then introduce the virus to urban cycles. For general information on mosquito transmission see mosquito transmission.
Diagnosis and management
Healthcare providers diagnose yellow fever by combining clinical suspicion with laboratory tests. Management emphasizes supportive care: fluid balance, treatment of bleeding, monitoring and management of organ failure. Intensive care may be required for severe cases. Early recognition improves outcomes and helps trigger public-health responses to reduce onward transmission.
Prevention and vaccination
A single dose of the live‑attenuated 17D vaccine produces long-lasting immunity in most people and is the primary prevention measure. Many countries require proof of vaccination for entry from endemic areas under international health regulations. Vaccination campaigns and routine childhood immunization are key components of control, supported by vector-control measures such as elimination of breeding sites and targeted insecticide use. Authoritative vaccination guidance is available from public-health agencies and vaccine information resources: vaccine information.
Geographic distribution and burden
Yellow fever is endemic in parts of sub-Saharan Africa and tropical South America. Gaps in immunization coverage and mosquito control can allow localized outbreaks. Global estimates from international public‑health bodies have indicated that tens to hundreds of thousands of symptomatic infections and thousands of deaths occur annually, although estimates vary by method and year; consult sources such as the World Health Organization for current burden estimates: WHO. Many national programmes focus on expanding coverage in affected regions, including countries in Africa and South America.
History and public-health impact
Yellow fever has been recognized for centuries and caused devastating urban epidemics in the 18th and 19th centuries in port cities of the Americas and elsewhere. The virus likely originated in Africa and was introduced to the Americas during the transatlantic slave trade. Development of the 17D vaccine in the 1930s greatly reduced epidemic risk. Historic outbreaks prompted early advances in mosquito control and in understanding mosquito-borne disease transmission.
Control strategies and readiness
- Vaccination: Routine immunization and mass campaigns in at-risk areas.
- Vector control: Reducing mosquito breeding sites, use of larvicides and adulticides where appropriate.
- Surveillance: Early detection of human cases and monitoring of viral activity in animal reservoirs.
- Travel advice: Vaccination before travel to endemic regions and mosquito protection measures.
Advice for travellers and clinicians
Prospective travellers to endemic or outbreak areas should seek vaccination and follow local public-health guidance. Clinicians should consider yellow fever in the differential diagnosis of febrile travellers with jaundice or hemorrhage and report suspected cases to public-health authorities promptly to enable contact tracing and targeted response.
For up-to-date and authoritative information consult national public-health agencies and international organizations such as the WHO, and reputable clinical guidance available through vaccine and infectious disease resources: vaccine, vector control and references on jaundice. Regional details are maintained by health authorities in Africa and South America.
Related articles
Author
AlegsaOnline.com Yellow fever: cause, transmission, prevention, and historical impact Leandro Alegsa
URL: https://en.alegsaonline.com/art/109761
Sources
- cdph.ca.gov : "Aedes Aegypti (Yellow Fever Mosquito) Fact Sheet"
- articles.philly.com : "yellow fever mosquito borne disease"