Testosterone: roles, synthesis, effects, and clinical significance
A comprehensive overview of testosterone: its biological synthesis, functions in males and females, physiological effects, clinical uses, disorders, and broader significance.
Overview
Testosterone is a steroid hormone that belongs to the class of male-type androgens. It is synthesized from cholesterol and circulates in the bloodstream bound to carrier proteins or free to enter cells. Although commonly described as a "male" hormone because of its prominent role in male development, testosterone is present and functional in people of all sexes, contributing to reproductive function, tissue growth and metabolic regulation.
Image gallery
8 Images






Production and biochemical pathway
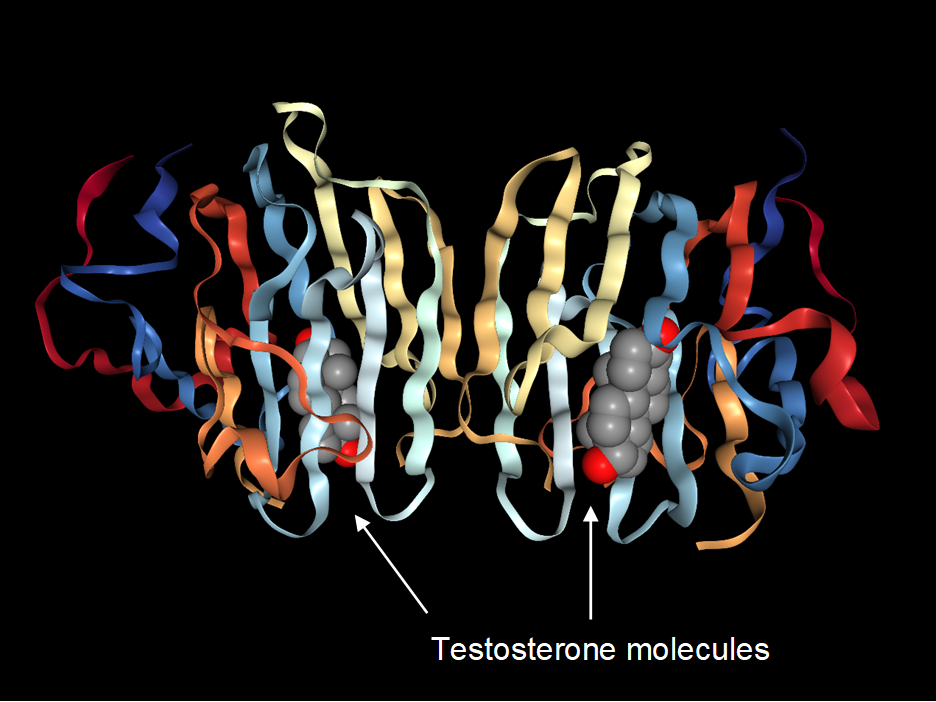
The principal sites of testosterone production are the testes in males and the ovaries in females; the adrenal glands also contribute small amounts. Synthesis begins with cholesterol and proceeds through several enzymatic steps in steroidogenic tissues. In certain target tissues testosterone is converted to the more potent androgen dihydrotestosterone (DHT) or aromatized to estradiol, a type of estrogen, which mediates some of testosterone's effects on bone and the brain. Testosterone acts primarily by binding the intracellular androgen receptor, influencing gene transcription, and producing longer-term ('genomic') and more rapid ('non-genomic') cellular effects.
Physiological effects and characteristics
Testosterone influences a wide range of body systems. Its effects are often grouped into anabolic (tissue-building) and androgenic (sex-characteristic) categories:
- Anabolic effects: promotion of skeletal muscle growth, bone density maintenance, and support of protein synthesis and nitrogen balance.
- Androgenic effects: development of male secondary sexual characteristics such as facial and body hair, deepening of the voice, growth of the external genitalia (for example the penis), and maturation of the reproductive tract.
Additional roles include support of libido and sexual function, stimulation of erythropoiesis (red blood cell production), influence on fat distribution, and effects on mood and cognition. Testosterone levels change across the life span—rising during puberty, peaking in early adulthood, and typically declining with age. Levels also show daily variation, often higher in the morning.
Clinical relevance, disorders and therapeutic use
Clinically, both low and high testosterone states are important. Hypogonadism refers to insufficient testosterone production and can cause fatigue, reduced sexual function, loss of muscle mass, and decreased bone density. Conversely, excess androgen action—whether from endogenous overproduction or from external anabolic steroid use—can produce virilization, menstrual disturbances in people assigned female at birth, and adverse metabolic effects.
Testosterone replacement therapy is used to treat confirmed hypogonadism and is available in several formulations, including injections, transdermal gels or patches, and oral or implanted preparations. Treatment decisions weigh potential benefits (improved energy, sexual function, bone and muscle) against risks; monitored parameters often include hematocrit, prostate health in men, and fertility considerations, because exogenous testosterone can suppress sperm production.
Historical notes and social context
Testosterone was isolated and characterized in the early 20th century, leading to medical uses and, later, the development of synthetic anabolic-androgenic steroids. These compounds have legitimate therapeutic roles but also a history of misuse for athletic performance and physique enhancement. Public health, ethical, and regulatory issues surround testing, prescribing, and non-medical use.
Important distinctions and notable facts
- Testosterone is one of several androgens; DHT and androgen precursors differ in potency and tissue specificity.
- Its functions overlap with estrogens in some tissues because of aromatization to estradiol.
- Laboratory measurement requires context: values vary by age, sex, time of day and assay method, so interpretation should be clinical rather than numeric alone.
For further reading on related biochemical pathways and clinical guidelines, see resources on androgens and sex hormones: androgens, sex hormone function, diagnostic testing for hormones, steroid biosynthesis from cholesterol, male physiology (male reproductive development), adrenal contributions (adrenal glands), and anatomy relevant to secondary sexual development (for example the penis).
Note: This article summarizes broadly accepted aspects of testosterone biology. Specific clinical decisions should rely on current medical guidelines and individualized assessment by qualified professionals.
Related articles
Author
AlegsaOnline.com Testosterone: roles, synthesis, effects, and clinical significance Leandro Alegsa
URL: https://en.alegsaonline.com/art/97217