Testicular cancer: overview, diagnosis, treatment, and prognosis
Testicular cancer affects one or both testicles, most often in males aged 15–40. It is usually highly treatable. This article covers types, symptoms, diagnosis, treatment, prognosis and fertility issues.
Overview
Testicular cancer is a malignant growth that arises in one or both testicles, the paired organs in the scrotum that produce sperm and testosterone. It is one of the less common cancers overall but is the most frequent cancer in younger adult men, with the highest incidence between roughly 15 and 40 years of age. Lifetime risk is low—for many populations about 1 in 250—and in high-resource settings cure rates exceed 90% when detected and managed appropriately.
Image gallery
5 Images



Types and anatomy
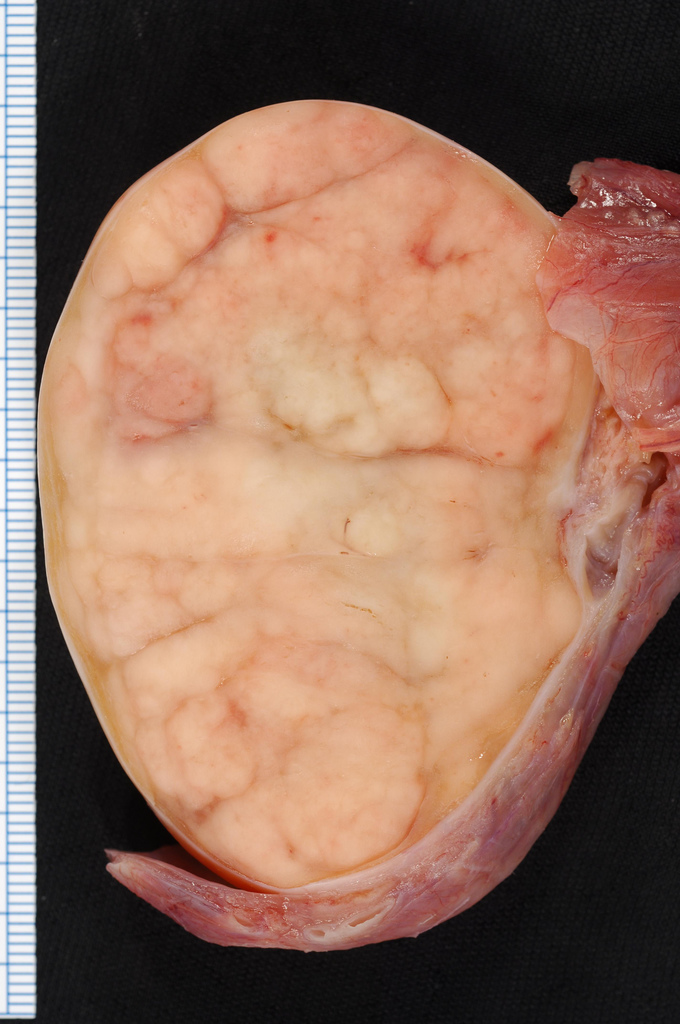
Most testicular cancers develop from germ cells, the sperm-forming cells. Germ cell tumors are broadly classified into two groups: seminomas and non-seminomas (which include embryonal carcinoma, yolk sac tumor, choriocarcinoma and teratoma). Less commonly they arise from stromal cells (Leydig or Sertoli cell tumors) or represent metastases from other sites. Understanding the type is important because it influences staging and treatment choices.
Signs, diagnosis and staging
Early disease often produces a painless lump or enlargement of the testicle. Other possible symptoms include a feeling of heaviness in the scrotum, dull ache in the groin or lower abdomen, or sudden scrotal pain. Evaluation typically begins with a physical exam and is followed by scrotal ultrasound to characterize a mass. Blood tests measure tumor markers such as alpha-fetoprotein (AFP), human chorionic gonadotropin (hCG) and lactate dehydrogenase (LDH), which assist diagnosis and monitoring. Imaging (CT or MRI) is used for staging to assess spread to lymph nodes or distant organs.
Treatment options
Treatment depends on tumor type and stage. Standard initial management for a suspicious testicular mass is radical inguinal orchiectomy (surgical removal of the affected testicle). Additional options include surveillance, retroperitoneal lymph node dissection, radiation therapy (more often used for seminoma), and platinum-based chemotherapy for more advanced disease. Many early-stage cases are managed with active surveillance after surgery to avoid overtreatment.
Prognosis, fertility and long-term issues
Testicular cancer has a very favorable prognosis compared with many other cancers. Cure rates exceed 90% overall, and even advanced cases often respond well to chemotherapy. However, treatment can affect fertility and hormone levels. Sperm banking before surgery or chemotherapy is commonly recommended if future fertility is a concern. Testosterone replacement may be needed if both testicles are removed or if hormonal function is impaired.
Risk factors, prevention and notable facts
- Recognized risk factors include a history of undescended testis (cryptorchidism), prior testicular cancer, family history, and certain genetic conditions.
- There is no proven population-wide screening program; regular self-examination can help early detection for individuals at higher risk.
- Because of excellent treatment outcomes, early recognition and prompt evaluation of testicular changes are particularly important.
For more general information on anatomy and reproductive health see male reproductive system. For detailed clinical guidance consult specialty resources or a urologist.
Related articles
Author
AlegsaOnline.com Testicular cancer: overview, diagnosis, treatment, and prognosis Leandro Alegsa
URL: https://en.alegsaonline.com/art/97212