Skull Bossing: Causes, Features, Diagnosis, and Management
Skull bossing is a prominence or enlargement of parts of the skull (commonly the forehead). Overview of causes, clinical features, investigation, treatment, and how it differs from other skull deformities.
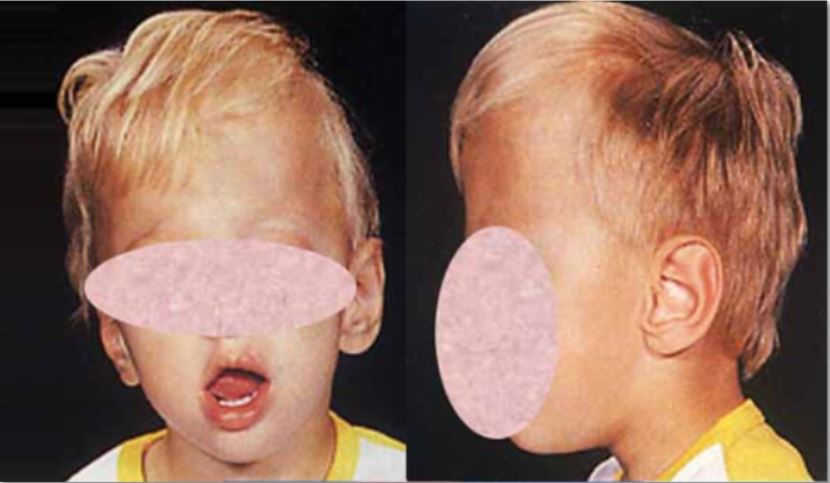
Skull bossing describes a visible prominence or overgrowth of one or more skull bones, most frequently affecting the forehead. In clinical usage the term frontal bossing is common when the frontal region is involved. The enlargement can be symmetrical or asymmetric and may be present at birth or develop later in life depending on the underlying condition.
Image gallery
4 Images


Causes and characteristic patterns
Multiple disorders can produce skull bossing by altering bone growth or stimulating marrow expansion. Typical causes include:
- Congenital and metabolic conditions — for example congenital hypothyroidism and childhood rickets, where impaired endocrine or mineral homeostasis changes skull shape.
- Hematologic diseases — chronic hemolytic anemias such as thalassemia may cause marrow hyperplasia and frontal and parietal bossing.
- Endocrine and bone disorders — acromegaly in adults and Paget disease of bone can produce thickening and prominence of cranial bones.
- Lysosomal storage disorders — some mucopolysaccharidoses lead to coarse facial features and skull prominence.
The raised area may represent true cortical bone overgrowth, thickening of the diploë, or expansion of marrow spaces. The frontal region is often highlighted in descriptions because the forehead is clinically conspicuous; the frontal bones can be referenced further via frontal bones.
Clinical assessment and important distinctions
Evaluation starts with a careful history and physical examination. Key questions include age at onset, associated developmental or endocrine signs, family history, and systemic symptoms. Important differential diagnoses include craniosynostosis (abnormal suture fusion), hydrocephalus, and generalized skull enlargement from metabolic bone disease.
- Investigations — plain skull radiographs, computed tomography for bone detail, and targeted laboratory tests (thyroid function, vitamin D, hemoglobin studies, growth hormone/IGF-1) help identify the cause.
- Treatment — directed at the underlying disorder: endocrine replacement, correction of nutritional deficiencies, transfusion and chelation strategies for thalassemia, or specific medical therapy for Paget disease. Surgical correction may be considered for cosmetic or functional problems.
Recognizing skull bossing is clinically useful because it can be an external clue to systemic disease. Management depends on accurate diagnosis and interdisciplinary care involving pediatrics, endocrinology, hematology, genetics and, when needed, craniofacial surgery.
Related articles
Author
AlegsaOnline.com Skull Bossing: Causes, Features, Diagnosis, and Management Leandro Alegsa
URL: https://en.alegsaonline.com/art/90972
Sources
- ncbi.nlm.nih.gov : PubMed Health: Frontal bossing
- ncbi.nlm.nih.gov : PMID 23049386