Pleurisy (pleuritis): inflammation of the pleural lining
Pleurisy, or pleuritis, is inflammation of the pleura that causes sharp, breathing-related chest pain. Causes include infections, embolism, autoimmune disease and malignancy; diagnosis and treatment target the cause.
Overview
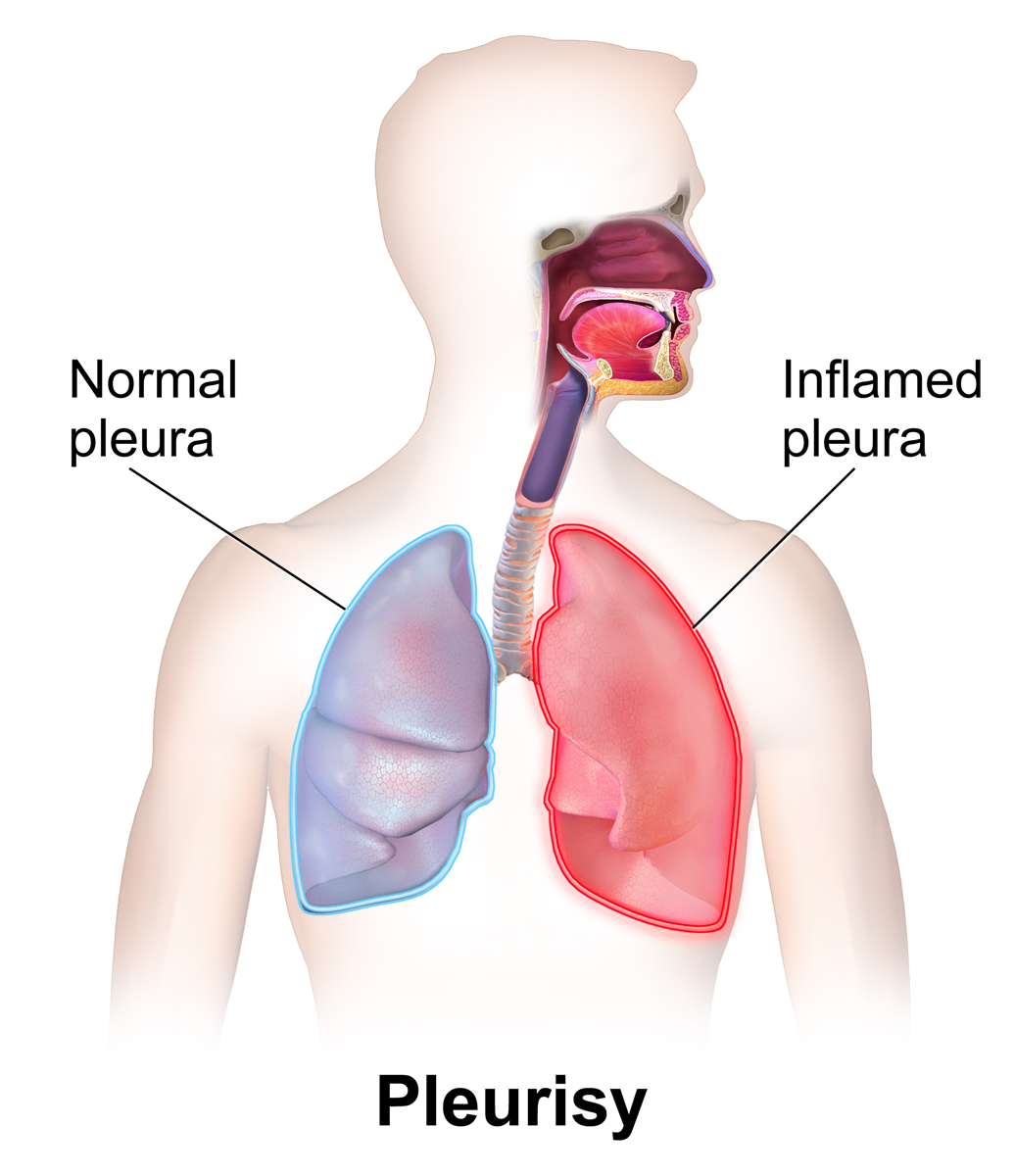
Pleurisy, also called pleuritis, is inflammation of the thin membranes that surround the lungs. Medically speaking it is an inflammatory process of the pleura, the dual-layered tissue that helps the lungs move smoothly in the chest. When these layers become inflamed they can rub together and produce distinctive pain and other respiratory symptoms.
Image gallery
2 Images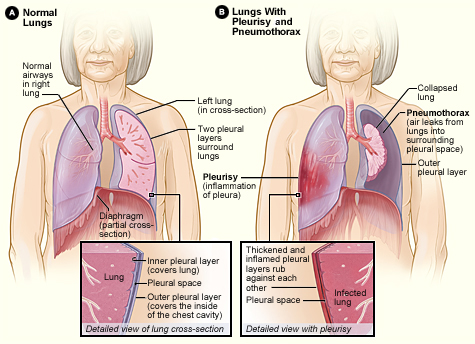
Anatomy and symptoms
The pleura consists of a visceral layer covering the lungs and a parietal layer lining the chest wall; the small space between them normally contains a thin film of fluid. Irritation or infection of these surfaces leads to sharp, often one-sided chest pain that worsens with breathing, coughing or deep inspiration. This is commonly known as pleuritic chest pain. Physical examination may reveal a pleural friction rub—an audible scratchy sound—or signs related to an associated pleural effusion (fluid accumulation).
Common causes
- Viral infections are among the most frequent causes, with inflammation spreading from lung tissues.
- Bacterial pneumonia can cause pleurisy and sometimes a complicated effusion or empyema.
- Pulmonary embolism often produces sudden pleuritic pain.
- Autoimmune diseases (for example rheumatoid arthritis or lupus), chest trauma, thoracic surgery, and cancers involving the pleura are other important causes.
Diagnosis
Evaluation begins with history and chest examination, followed by imaging such as chest X‑ray, ultrasound or CT to look for effusion or lung disease. Blood tests and microbiology help identify infection or systemic causes. When fluid is present, thoracentesis (sampling of pleural fluid) and laboratory analysis guide management.
Treatment and prognosis
Management focuses on treating the underlying cause and relieving symptoms. Analgesics and anti-inflammatory medications can reduce pain; oxygen and rest support breathing. Bacterial infections require antibiotics; significant pleural effusions may need drainage. Recurrent malignant effusions or persistent symptoms sometimes require procedures to prevent fluid reaccumulation. Most acute cases improve once the cause is controlled, but complications such as empyema or chronic pleural thickening can occur.
Distinctions and notable points
Pleuritic pain is classically sharp and movement-dependent, which helps distinguish it from cardiac ischemic pain that is often pressure-like and exertional. Because multiple conditions can produce pleurisy, a careful assessment is important. For general information about the pleural membranes and respiratory anatomy, see the entry on the pleura and lung lining.
Related articles
Author
AlegsaOnline.com Pleurisy (pleuritis): inflammation of the pleural lining Leandro Alegsa
URL: https://en.alegsaonline.com/art/77466
Sources
- cedars-sinai.edu : Cedars-Sinai: Pleurisy.
- merckmanuals.com : The Merck Manual Home Health Handbook: Viral Pleuritis.