Helicobacter pylori: biology, disease, diagnosis and treatment
Helicobacter pylori is a spiral, urease-producing bacterium that colonizes the stomach lining and is a major cause of gastritis and peptic ulcers. This article covers its biology, clinical importance and management.
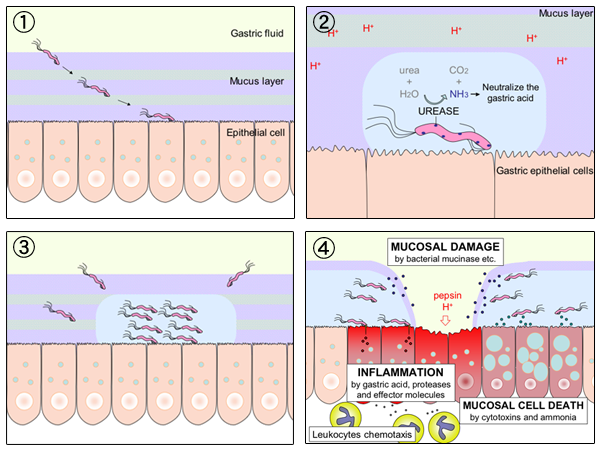
Helicobacter pylori is a Gram-negative, spiral-shaped bacterium adapted to live on the mucous layer that coats the stomach. It produces large amounts of the enzyme urease, which neutralizes gastric acid locally and helps the organism survive in an acidic environment. H. pylori is a leading cause of chronic gastritis and a major contributor to peptic ulcer disease; it is found on the lining of the stomach and can damage the protective mucosa, permitting ulcers to form. It is also associated with an increased risk of gastric cancer and mucosa-associated lymphoid tissue (MALT) lymphoma.
Image gallery
6 Images



Characteristics and laboratory features
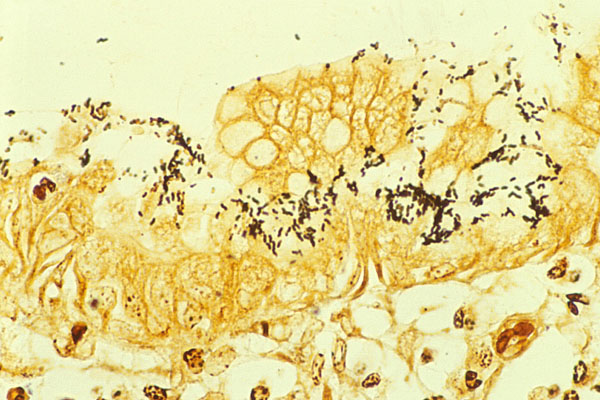
H. pylori is microaerophilic (requiring reduced oxygen) and motile, using flagella to penetrate mucus. Its spiral shape and motility facilitate movement through viscous gastric mucus. The bacterium is strongly urease-positive, which is the basis for several diagnostic tests: urease activity hydrolyzes urea to ammonia and carbon dioxide, creating a local alkaline microenvironment. Under microscopes and on culture, H. pylori shows characteristic curved rods; however, culture can be difficult and requires special conditions.
Clinical importance and complications
Infection commonly causes chronic inflammation of the stomach (gastritis). Persistent infection increases the likelihood of peptic ulcers in the stomach or the first part of the small intestine, the duodenum, and is implicated in many cases of peptic ulcer disease (peptic ulcers). Long-standing infection is a recognized risk factor for gastric adenocarcinoma. Symptoms of active disease may include epigastric pain, nausea, bloating and, in complicated cases, bleeding.
Diagnosis and treatment
Testing may be noninvasive or invasive. Common noninvasive options include the urea breath test and stool antigen test; invasive testing involves endoscopy with biopsy for histology, rapid urease testing or culture. Typical treatment aims to eradicate the bacterium and reduce acid: regimens combine two effective antibiotics with an acid-suppressing proton pump inhibitor, and sometimes bismuth compounds. Rising antibiotic resistance has made choice of regimen and confirmation of eradication increasingly important.
Transmission, prevalence and prevention
H. pylori is usually acquired in childhood and is transmitted by oral–oral or fecal–oral routes; crowded living conditions and limited sanitation increase transmission. Prevalence varies widely by region and by socioeconomic factors. Eradication of active infection reduces ulcer recurrence and may decrease the risk of some gastric cancers, which is why targeted testing and treatment strategies are used in many clinical guidelines.
History and notable facts
The bacterium was identified by Australian researchers Barry J. Marshall and J. Robin Warren, who demonstrated its role in gastritis and peptic ulcer disease and were awarded the Nobel Prize in Physiology or Medicine in 2005. Before their work, peptic ulcers were commonly attributed to diet, stress or excess gastric acid; since the discovery, medical practice has shifted to antibiotic-based cures and prevention strategies (pre-discovery beliefs). For more on discovery and background see foundational accounts by the original investigators and subsequent reviews (Marshall & Warren).
- Small intestine (context for duodenal disease)
- Peptic ulcer disease overview
- Gastric mucosa and colonization
Current practice emphasizes accurate diagnosis, appropriate antibiotic selection informed by local resistance patterns, and confirmation of eradication after therapy. Ongoing research explores vaccines, improved diagnostic tools and strategies to manage antibiotic resistance.
Questions and answers
Q: What is Helicobacter pylori?
A: Helicobacter pylori is a bacterium that has a spiral shape and is found in the stomach or on its lining.
Q: What is the cause of more than 90 percent of ulcers?
A: H. pylori is the cause of more than 90 percent of ulcers, which are sores found in the lining of the stomach or the duodenum.
Q: What did doctors believe was the cause of most ulcers before 1982?
A: Before 1982, doctors thought that spicy food, acid, stress, and lifestyle caused most ulcers.
Q: How can most ulcers be cured now?
A: Doctors now know that most ulcers are caused by an H. pylori infection, and they can be cured with the correct antibiotics.
Q: Who were the scientists who discovered H. pylori, and what prize did they win for their work?
A: Australian scientists Barry J. Marshall and J. Robin Warren were the first to discover H. pylori, and they won the Nobel Prize in Physiology or Medicine in 2005 for their work.
Q: What is the duodenum?
A: The duodenum is the first part of the small intestine.
Q: What are the symptoms of an H. pylori infection?
A: Common symptoms of an H. pylori infection include stomach pain, bloating, nausea, vomiting, and loss of appetite. However, some people with an H. pylori infection may not experience any symptoms at all.
Related articles
Author
AlegsaOnline.com Helicobacter pylori: biology, disease, diagnosis and treatment Leandro Alegsa
URL: https://en.alegsaonline.com/art/43352