Adrenal tumor (adrenal mass): overview, types, diagnosis and management
Adrenal tumors are growths in the adrenal glands that may be benign or malignant and can alter hormone production. This article explains types, symptoms, diagnosis, treatment and important clinical distinctions.
An adrenal tumor, also called an adrenal mass, is an abnormal growth arising in one of the two adrenal glands that sit above the kidneys. These growths range from harmless, non‑functioning nodules found incidentally to aggressive cancers and hormone‑secreting lesions that cause systemic illness. Whether a tumor produces hormones is a key factor determining symptoms, diagnostic steps and treatment.
Image gallery
4 Images


Types and anatomy
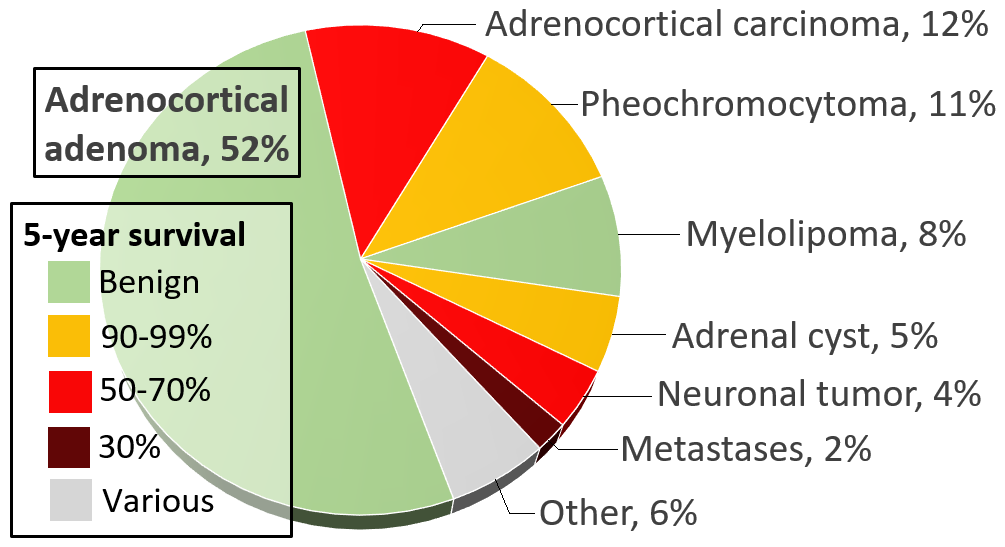
The adrenal gland has two major parts: the outer cortex and the inner medulla. Tumors are commonly classified by their cell of origin and behavior. Examples include:
- Cortical adenomas: usually benign and may be non‑functional or secrete cortisol or aldosterone (benign).
- Adrenocortical carcinoma: a rare, often aggressive cancer occurring in the cortex (malignant).
- Pheochromocytoma: medullary tumors that produce catecholamines; most are benign but some behave malignantly (adrenal gland related).
- Neuroblastoma: primarily a pediatric malignancy that can involve the adrenal medulla (neuroblastoma).
Clinical features
Symptoms depend on hormone production and size. Functional tumors may cause Cushingoid features, resistant hypertension from excess aldosterone, episodes of headache, palpitations and sweating from catecholamine excess, or signs of virilization from androgen secretion. Nonfunctional masses are often asymptomatic and discovered incidentally on imaging.
Diagnosis
Evaluation combines biochemical testing and imaging. Tests look for excess cortisol, aldosterone, or catecholamine metabolites; biochemical screening helps avoid dangerous procedures when a pheochromocytoma is suspected (endocrine hormones). Cross‑sectional imaging with CT or MRI defines size and appearance. Nuclear medicine scans and functional imaging may be used for specific tumor types or to detect metastatic disease. Percutaneous biopsy is infrequently used and generally avoided if a hormonally active tumor is suspected (metastasize).
Treatment and prognosis
Management is tailored to tumor type and activity. Surgical removal is the cornerstone for most localized tumors, often after medical stabilization of hormone excess. Nonoperative approaches include medical therapy to control hormones, targeted agents or systemic therapy for metastatic cancer, and surveillance for small, nonfunctioning incidentalomas. Prognosis varies widely: benign adenomas have an excellent outlook, while adrenocortical carcinoma and metastatic disease require more aggressive treatment and carry a higher risk.
Understanding the distinction between cortical and medullary tumors, between functional and nonfunctional lesions, and between primary and metastatic adrenal disease is crucial for safe care. For additional clinical resources and guidelines see benign, malignant and specialty links such as adrenal gland, endocrine hormones, neuroblastoma and metastasize.
Related articles
Author
AlegsaOnline.com Adrenal tumor (adrenal mass): overview, types, diagnosis and management Leandro Alegsa
URL: https://en.alegsaonline.com/art/1065
Sources
- thehindu.com : "Doctors remove 'world's largest adrenal tumour'"