Thyroid cancer: types, diagnosis, treatment, and prognosis
Concise encyclopedia overview of thyroid cancer covering the gland, major types, causes, diagnosis, treatments, outcomes, and notable distinctions.
Thyroid cancer is a disease in which abnormal cells form in the tissues of the thyroid, a small gland at the base of the neck that regulates metabolism through hormones. It ranges from slow-growing forms that are highly treatable to aggressive variants with poorer outcomes. Patients commonly discover a lump or swelling in the neck, though many cases are detected incidentally on imaging. For more context, see Thyroid cancer.
Image gallery
3 Images
Types and characteristics
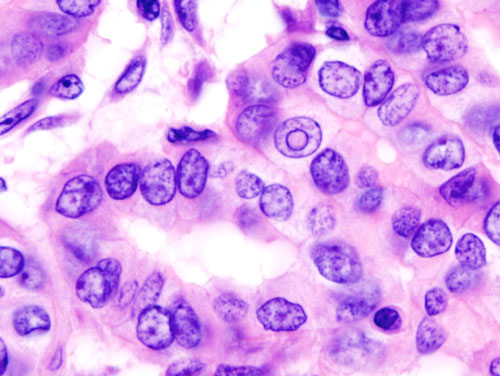
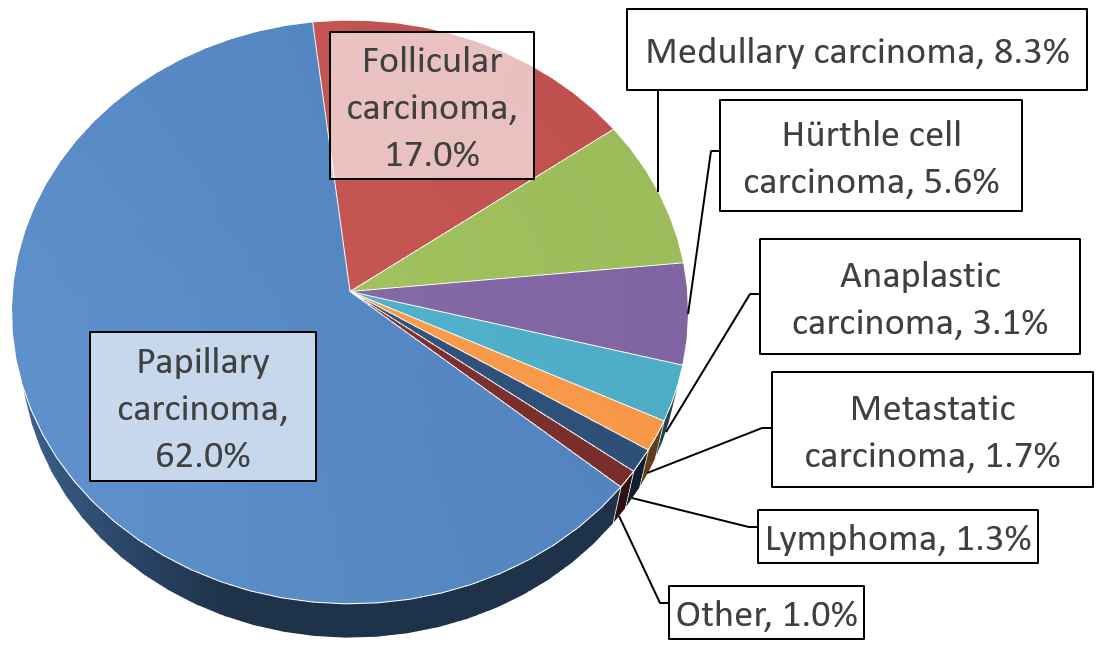
Pathologists classify thyroid cancers by the type of cell involved and how the tumor looks under the microscope. Major categories include:
- Papillary: the most frequent form, often slow-growing and with a good prognosis.
- Follicular: similar behavior to papillary in many cases, sometimes spreads to bone or lung.
- Medullary: arises from parafollicular (C) cells and can be hereditary; it requires distinct genetic evaluation.
- Anaplastic: rare but very aggressive, usually occurring in older adults.
Diagnosis
Evaluation typically begins with a physical exam and ultrasound of the thyroid. Suspicious nodules are sampled by fine-needle aspiration biopsy for cytology. Blood tests assess thyroid function and, in some cases, tumor markers. Cross-sectional imaging and nuclear medicine scans help stage disease and detect spread when needed.
Treatment and management
Treatment choices depend on tumor type, stage, patient age and health. Common approaches include:
- Surgery (partial or total thyroidectomy) to remove the primary tumor.
- Radioactive iodine therapy for certain differentiated cancers to ablate remaining tissue.
- Thyroid hormone replacement and suppression therapy to lower stimulation of any remaining cancer cells.
- Targeted therapies, external radiation, or chemotherapy for advanced, recurrent, or anaplastic disease.
Post-treatment follow-up is important and often includes neck ultrasound and measurement of tumor markers (for example, thyroglobulin for differentiated cancers). Long-term surveillance helps detect recurrence early.
Risk factors include prior radiation exposure to the head or neck, certain inherited syndromes (notably for medullary cancer), female sex, and some environmental influences. Prognosis is generally favorable for the common differentiated types when diagnosed and treated appropriately, while rarer subtypes require more aggressive care. Multidisciplinary teams — surgeons, endocrinologists, pathologists, radiologists and oncologists — commonly collaborate to optimize outcomes.
Related articles
Author
AlegsaOnline.com Thyroid cancer: types, diagnosis, treatment, and prognosis Leandro Alegsa
URL: https://en.alegsaonline.com/art/99751
Sources
- my.clevelandclinic.org : "Thyroid Cancer"
- health.com : "Sofia Vergara Beats Thyroid Cancer"
- well.blogs.nytimes.com : "The Workout: Sofia Vergara Hates to Exercise"