Staphylococcus aureus
A common Gram-positive bacterium that colonizes humans and causes a range of diseases from skin infections to life‑threatening invasive illness; notable for antibiotic resistance and virulence factors.
Overview
Staphylococcus aureus (S. aureus) is a spherical, Gram-positive bacterium frequently found on human skin and in the anterior nares (nostrils). Cells typically appear in irregular, grape-like clusters when viewed microscopically and form characteristic gold-tinged colonies on some culture media, a trait reflected in the species name aureus (Latin for "golden"). S. aureus is a facultative anaerobe capable of growing with or without oxygen and is a common component of the human microbiota. Although often harmless when carried asymptomatically, it can act as an opportunistic pathogen and cause a wide range of clinical conditions.
Image gallery
10 Images








Biology and laboratory identification
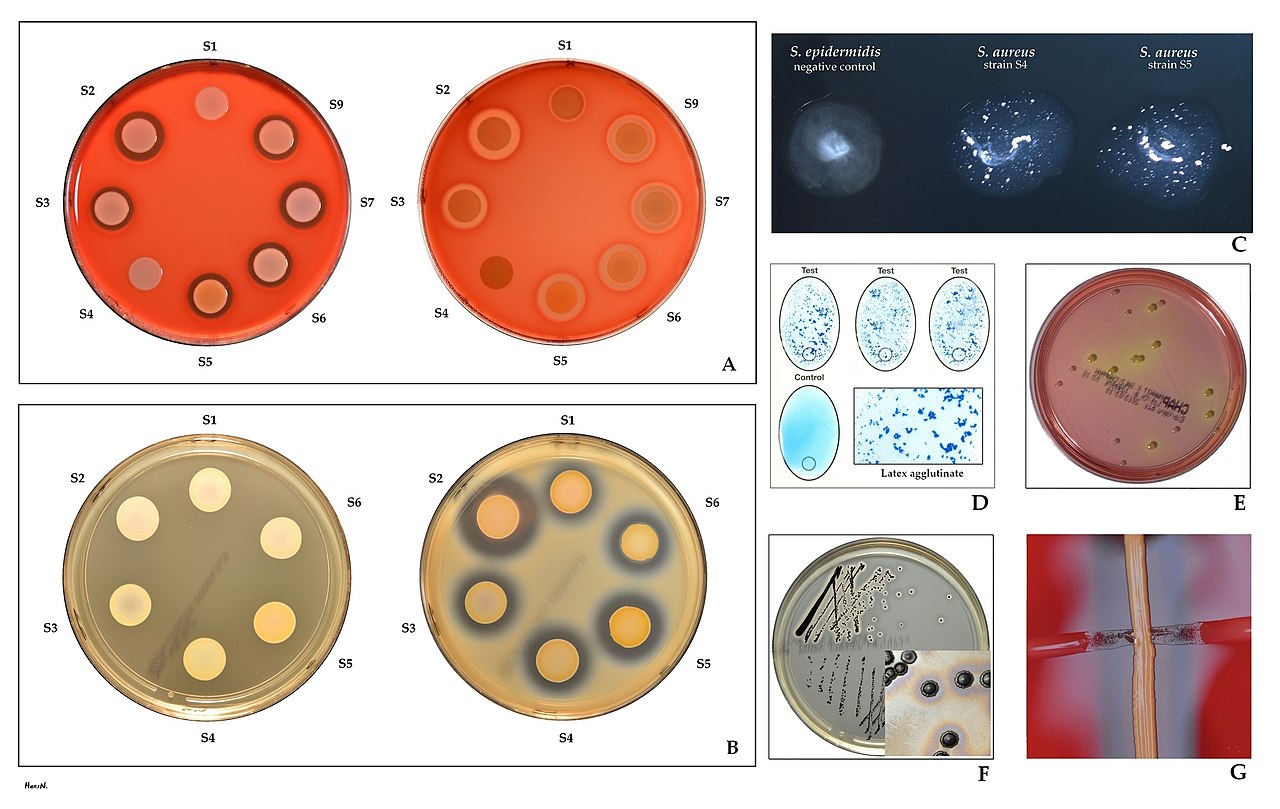
Laboratory identification is based on morphology, staining and biochemical behavior. S. aureus is catalase-positive and usually coagulase-positive, which helps distinguish it from other Staphylococcus species. On blood agar the organism often produces beta-hemolysis, and colonies may show yellow-to-golden pigmentation. Diagnostic tests in clinical microbiology include Gram staining, culture, catalase and coagulase assays, and modern methods such as mass spectrometry or molecular assays for rapid species-level confirmation.
Clinical significance and common manifestations
S. aureus causes a spectrum of disease ranging from localized skin and soft tissue infections (folliculitis, boils, impetigo, abscesses) to deeper or systemic illness including wound infections, osteomyelitis, septic arthritis, pneumonia, bacteremia and endocarditis. Certain strains produce toxins that produce distinct syndromes: enterotoxins can trigger rapid-onset food poisoning, toxic shock syndrome toxin-1 (TSST-1) can cause toxic shock syndrome, and other cytotoxins contribute to tissue damage. Invasive infections can be severe and require prompt medical attention.
Transmission, carriage and prevention
Transmission occurs mainly via direct contact with colonized or infected individuals, or indirectly through contaminated objects (fomites). The anterior nares and skin are primary sites of colonization; many people carry S. aureus without symptoms. Preventive measures in both community and healthcare settings include hand hygiene, appropriate wound care and environmental cleaning. In certain contexts, decolonization protocols (such as topical nasal mupirocin and antiseptic body washes) may be used to reduce carriage and lower infection risk.
Treatment and antibiotic resistance
Treatment depends on the infection type and antibiotic susceptibility. Historically, penicillin and related beta-lactam antibiotics were effective, but many strains acquired resistance through beta-lactamase production. Methicillin-resistant S. aureus (MRSA) emerged after methicillin was introduced and remains an important clinical challenge. MRSA strains are resistant to many beta-lactams and often require alternative agents such as vancomycin, linezolid or daptomycin; antimicrobial choice should be guided by susceptibility testing. There is currently no widely used vaccine against S. aureus.
History, epidemiology and notable distinctions
The bacterium was first described in the late 19th century and has been recognized as a major cause of human infection since that time. Its ability to live harmlessly on hosts while retaining the capacity to invade tissues has contributed to its persistence in communities and healthcare facilities. Clinically and epidemiologically important distinctions include hospital-acquired versus community-associated strains, which differ in resistance patterns and typical presentations. Some virulence factors, such as protein A, various hemolysins and Panton–Valentine leukocidin (PVL), are often discussed in relation to disease severity, though the contribution of individual factors varies among strains.
Further information
- Common clinical contexts: skin and soft tissue infections, surgical site infections, bloodstream infections.
- Key laboratory tests: Gram stain, culture, catalase and coagulase tests, susceptibility testing.
- Prevention focus: hand hygiene, contact precautions in healthcare settings, careful antibiotic stewardship to limit resistance.
For an overview of clinical guidance and laboratory methods, see additional resources and institutional protocols. For specific cases, treatment should always be tailored by clinicians using up-to-date susceptibility data and expert recommendations.
Related articles
Author
AlegsaOnline.com Staphylococcus aureus Leandro Alegsa
URL: https://en.alegsaonline.com/art/93411
Sources
- commons.wikimedia.org : Staphylococcus aureus