Scoliosis: overview, causes, diagnosis, and management
Scoliosis is a lateral curvature of the spine that ranges from mild cosmetic asymmetry to severe deformity affecting function and breathing. Causes include idiopathic, congenital, neuromuscular, and degenerative forms.
Scoliosis is a condition in which the spine deviates laterally from its normal vertical alignment when viewed from behind, producing an S-shaped or C-shaped curve. The term covers a range of spinal curvatures that vary in size, location and cause. Curves may remain stable for years or progress, particularly during periods of rapid growth. Mild scoliosis often requires only monitoring; larger or progressive curves can cause back pain, altered posture, reduced chest capacity and, in severe cases, impaired respiratory function.
Image gallery
9 Images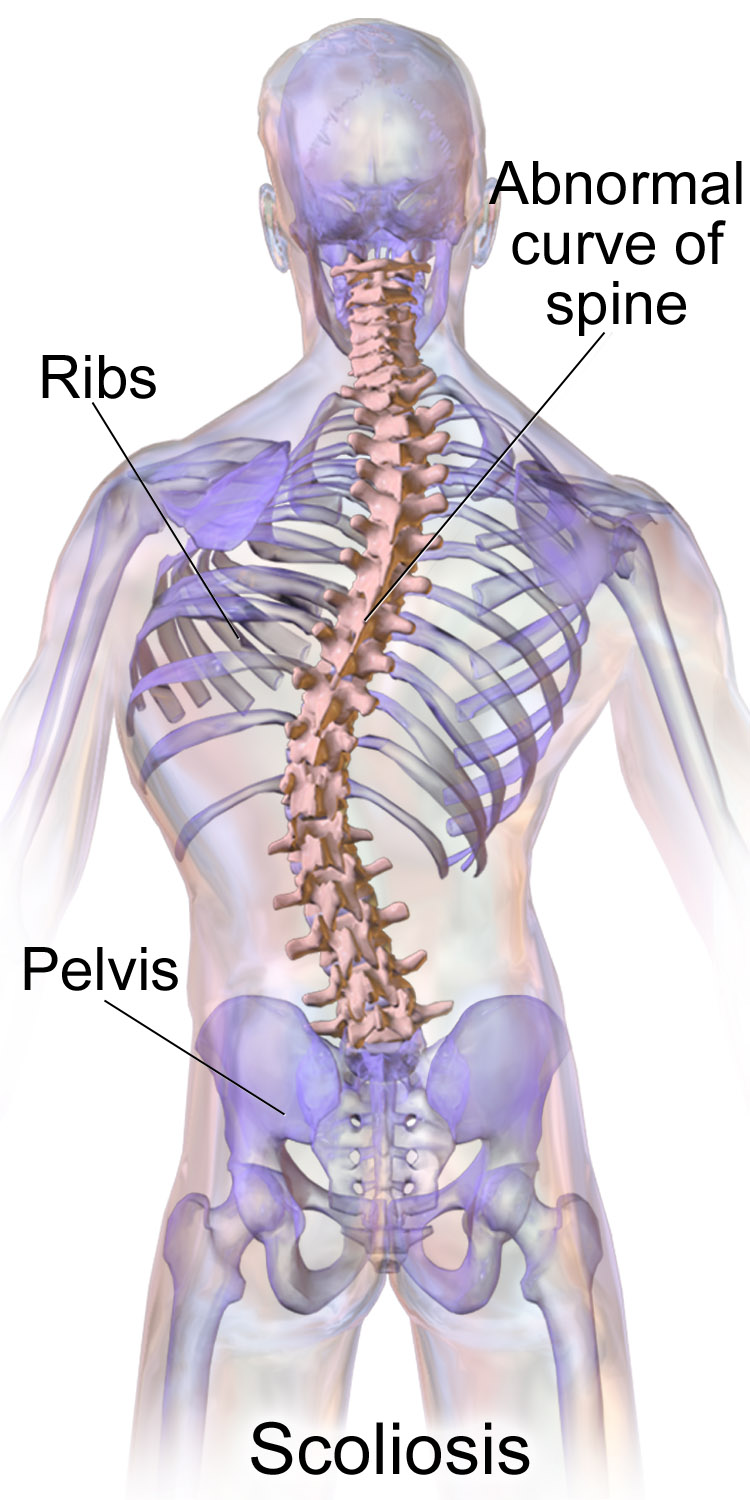







Classification and causes
Scoliosis is commonly classified by age at onset and underlying cause. Major categories include:
- Idiopathic scoliosis — the most frequent type, especially in adolescents, where no single cause is identified.
- Congenital scoliosis — caused by vertebral malformations present at birth.
- Neuromuscular scoliosis — associated with conditions such as cerebral palsy, muscular dystrophy or spinal cord injury that affect muscle control.
- Degenerative (adult) scoliosis — develops from wear and tear of the spinal joints and discs later in life.
Evidence indicates a contribution from inherited factors to susceptibility in many cases, and studies examine genetic components alongside non‑genetic and environmental influences. A family history of scoliosis increases the risk of occurrence or progression, but the precise mechanisms are complex and incompletely understood.
Who is affected
Scoliosis most often becomes apparent during the rapid growth of adolescence, commonly between about 10 and 18 years of age, though onset can occur earlier or later. Females are more likely than males to develop curves that progress and require treatment. A small percentage of children and adolescents show structural scoliosis; in adults, degenerative scoliosis is more often linked to aging of spinal structures.
Signs and diagnosis
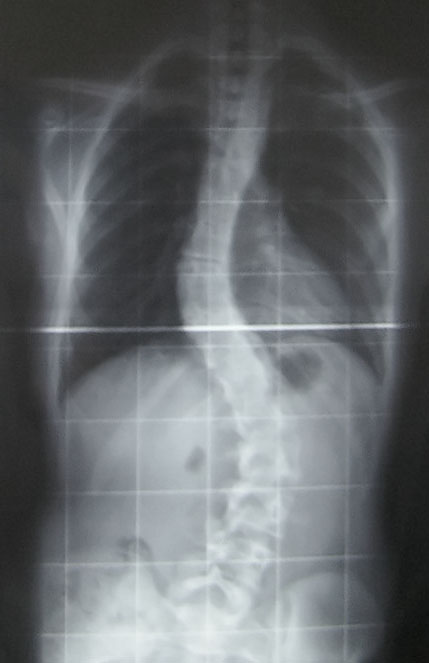
Initial recognition frequently follows observation of body asymmetry. Common clinical signs include uneven shoulders or hips, a rib prominence on one side that appears when bending forward (Adam's test), and a visible lean. Primary assessment is clinical; definitive evaluation uses standing radiographs to measure the Cobb angle, describe curve pattern and assess skeletal maturity. Advanced imaging such as MRI is used when neurologic symptoms, congenital anomalies or atypical features suggest spinal cord or soft‑tissue involvement. For general descriptions of spinal anatomy and curve assessment see resources on the human spine, comparative material on the animal spine, and specialist summaries of curve assessment.
Treatment and management
Management is individualized according to curve size, progression risk, age and symptoms. Common approaches include:
- Observation — periodic clinical and radiographic follow‑up for small, non‑progressing curves.
- Bracing — used in growing adolescents with moderate curves to reduce the risk of progression; effectiveness depends on fit, type and adherence.
- Physical therapy and exercise — programs including scoliosis‑specific exercises can support posture, function and pain management, though they do not replace other interventions when indicated.
- Surgery — considered for large, symptomatic or rapidly progressing curves; spinal fusion with instrumentation is the most common procedure, with contemporary techniques focused on correcting alignment and maintaining balance while minimizing complications.
Decisions balance the risks and benefits of intervention against the likely natural history of a given curve. Thresholds for surgery depend on multiple factors, including Cobb angle, symptoms and growth potential; multidisciplinary assessment is recommended.
Prognosis, screening and impact
Many small curves remain stable and cause little disability. Progressive or severe thoracic curves are more likely to affect respiratory function and quality of life. Screening programs for adolescents have been implemented in some areas but are debated because of variable evidence on long‑term benefit, the potential for false positives and resource implications. Beyond physical effects, visible deformity may have psychosocial consequences, so care often includes attention to emotional and social wellbeing.
Ongoing research continues into genetic risk factors, improved brace designs, less invasive surgical approaches and methods to predict which curves will progress. For authoritative clinical guidance and up‑to‑date research summaries consult professional societies and specialist centers through the references noted above.
Related articles
Author
AlegsaOnline.com Scoliosis: overview, causes, diagnosis, and management Leandro Alegsa
URL: https://en.alegsaonline.com/art/88061
Sources
- niams.nih.gov : "Scoliosis in Children and Adolescents"
- ghr.nlm.nih.gov : "Adolescent Scoliosis"