Human T-lymphotropic virus (HTLV)
Overview of the Human T-lymphotropic viruses: classification, biology, clinical significance, transmission, history, and prevention.
Overview
Human T-lymphotropic viruses (commonly abbreviated HTLV) are a group of closely related human retroviruses that primarily infect T lymphocytes. They are known for their ability to integrate into host DNA and for causing a range of long-term conditions in a minority of infected people, most notably adult T-cell leukemia/lymphoma and certain chronic inflammatory disorders. For a general introduction see Human T-lymphotropic virus.
Image gallery
2 Images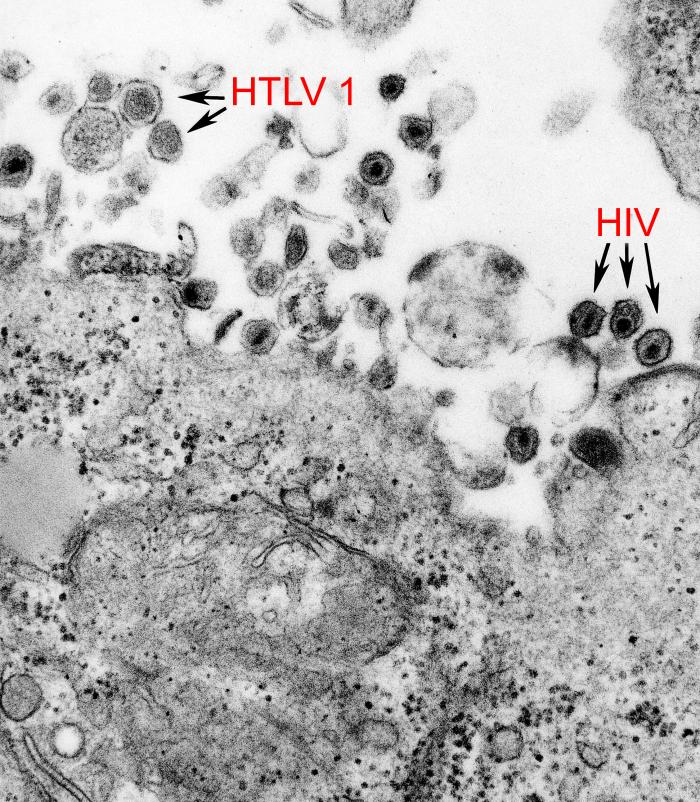

Biology and classification
HTLV viruses belong to the retrovirus family and are classified among deltaretroviruses. Like other retroviruses, they carry RNA genomes and use reverse transcriptase to form DNA copies that integrate into the host cell genome as a provirus. HTLV targets T cells, especially CD4+ lymphocytes, and can persist lifelong in infected individuals. Four types have been described in humans: HTLV-1, HTLV-2, HTLV-3 and HTLV-4. The first two are the best characterized; HTLV-3 and HTLV-4 were more recently identified in limited numbers and appear to be related to simian viruses.
Clinical importance
Most people infected with HTLV remain asymptomatic. However, HTLV-1 is the established cause of adult T-cell leukemia/lymphoma (ATLL) and of a progressive neurologic condition called HTLV-1–associated myelopathy/tropical spastic paraparesis (HAM/TSP). HTLV-2 has occasionally been linked to neurologic and hematologic disorders but is generally associated with milder disease. HTLV-associated illnesses can take years or decades to develop after infection. See also discussions of retroviral oncogenesis and leukemia for context: retrovirus and leukemia.
Transmission and prevention
- Transmission occurs through infected blood and blood products, sexual contact, sharing of needles, and from mother to child—especially via breastfeeding.
- Prevention strategies include screening blood donors, counseling for people known to be infected, safer-sex practices, harm reduction for injection drug use, and alternatives to breastfeeding when maternal infection is known.
History and distribution
HTLV-1 was the first human retrovirus identified and was recognized in the late 20th century. Subsequent studies linked it to both leukemia and chronic neurologic disease. HTLV-1 is unevenly distributed worldwide and is endemic in regions such as southwestern Japan, parts of the Caribbean, several areas of Africa and South America. HTLV-2 is found among some indigenous populations and in people with a history of injection drug use. HTLV-3 and HTLV-4 were identified more recently in small numbers of people in central Africa and appear to have arisen through cross-species transmission from primates.
Diagnosis, management and notable facts
Diagnosis is typically made by detecting antibodies to the virus or by molecular tests that identify proviral DNA. There is no single curative antiviral therapy that reliably clears HTLV infection; clinical care focuses on treating complications such as ATLL or managing progressive neurologic impairment. Public health measures, especially blood screening and education, have reduced transmission risk in many settings. HTLV is distinct from HIV despite some superficial similarities: they are different genera of retroviruses with different disease profiles and clinical courses.
Related articles
Author
AlegsaOnline.com Human T-lymphotropic virus (HTLV) Leandro Alegsa
URL: https://en.alegsaonline.com/art/45672