Hyperglycemia — high blood sugar: causes, symptoms, diagnosis, treatment
Hyperglycemia is elevated blood glucose. This article explains causes, signs, testing, acute dangers, long-term complications, treatment and prevention in clear, practical terms.
Overview
Hyperglycemia refers to higher-than-normal levels of glucose in the bloodstream. When circulating glucose remains elevated, body tissues and organs can be harmed over time. In clinical practice, certain numeric thresholds are used to identify hyperglycemia, and very high readings are a hallmark of diabetes mellitus. Acute severe hyperglycemia can be life-threatening if not recognised and treated promptly.
Image gallery
3 Images

How it develops
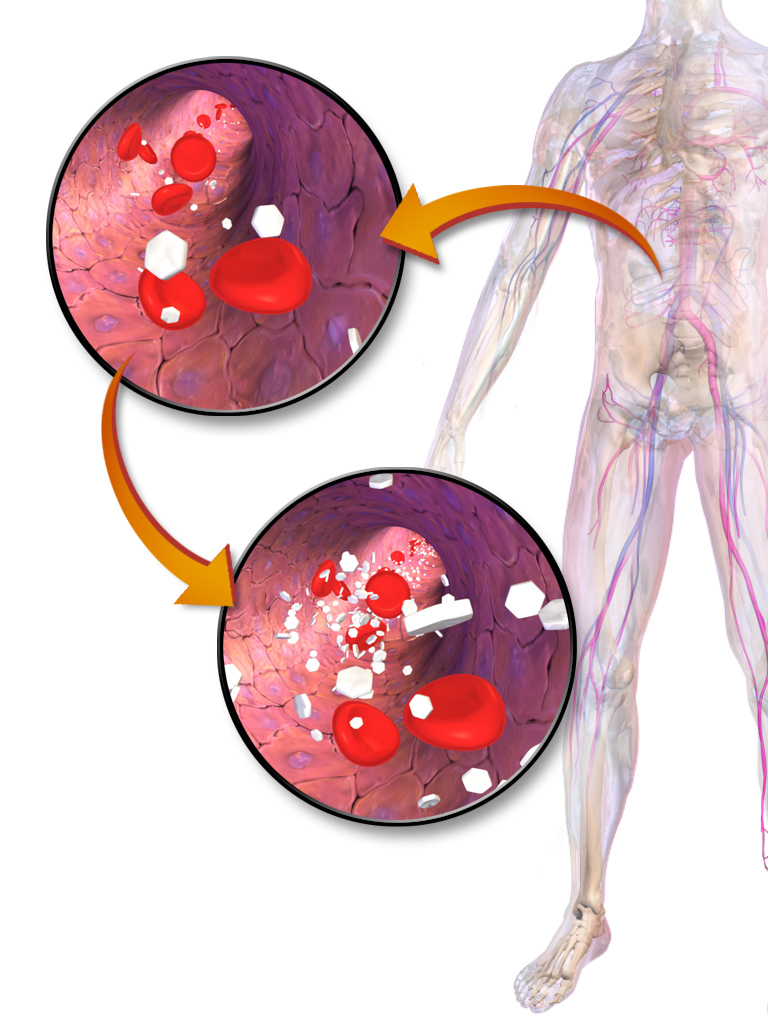
Blood glucose normally moves from the vascular space into body cells where it becomes fuel. This transfer depends on the hormone insulin resistance when cells fail to respond to insulin, or on a shortage of insulin itself. Insulin helps glucose — commonly called sugar — enter cells so those cells can make energy. If insulin action is insufficient, excess glucose remains in the blood and produces the pattern called hyperglycemia. Causes include inadequate insulin production, medication effects, stress hormones during illness, certain endocrine disorders, and lifestyle factors.
Common causes and risk factors
- Type 1 and type 2 diabetes, the most frequent underlying conditions.
- Missed or inadequate doses of glucose-lowering medication or insulin.
- Acute infection, surgery, or severe illness that raise stress hormones.
- Certain drugs such as corticosteroids or some psychiatric medicines.
- Poor dietary control, inactivity, and obesity linked to insulin resistance.
Signs, testing and diagnosis
Early symptoms may be subtle: increased thirst, frequent urination, fatigue, blurred vision and slow wound healing. More pronounced hyperglycemia often produces dry mouth and weakness. Clinicians confirm elevated glucose with blood tests — fingerstick glucose monitoring or laboratory plasma measurements — and consider patterns over time. Persistent or recurrent high readings often prompt evaluation for diabetes mellitus or other contributing disorders.
Acute complications
Very high blood sugar can lead to emergencies such as diabetic ketoacidosis and hyperosmolar hyperglycemic state; these events cause dehydration, altered consciousness and metabolic disturbance and require urgent care. Repeated hyperglycemia also increases risk of cardiovascular disease, nerve damage, kidney injury and eye disease. Controlling blood glucose reduces these long-term risks.
Treatment and prevention
Management aims to lower glucose safely and address the underlying cause. For people with diabetes this commonly includes lifestyle measures (diet, physical activity), oral medications or injectable insulin. Sick-day plans, regular self-monitoring and adjustment of therapy are important to prevent severe elevations. In emergency situations, intravenous fluids and insulin are used along with treatment of precipitating illness.
Practical points and distinctions
Not every transient high reading signifies chronic disease; stress, recent meals and some medicines can temporarily raise levels. The distinction between random short-lived elevations and established hyperglycemia that meets diagnostic criteria for diabetes is made using standardized tests and clinical assessment. Simple patient education—how to test blood glucose, recognise danger signs and when to seek help—can prevent many complications. For more detailed guidance and local resources consult professional health information and care teams via your usual channels, or follow trusted clinical resources such as national diabetes associations and health services (health information). Additional reading on related topics: glucose metabolism (cellular glucose handling), the role of the bloodstream in transport (blood), and why insulin matters (insulin resistance). Other useful topics include emergency signs of severe hyperglycemia (symptoms of high sugar) and the diagnosis of diabetes (glucose testing).
For urgent concerns about prolonged or very high readings, seek immediate medical evaluation. Early recognition and consistent management are the most effective ways to reduce the short- and long-term harms of hyperglycemia.
Occurrence
The blood glucose level in healthy people should be below 100 mg/dl when fasting (i.e. at least 8 hours after the last calorie intake) and below 140 mg/dl after a sugar load test. When the body consumes food, glucose and other sugars, with a few exceptions, are absorbed through the intestine and passed through the portal vein (enterohepatic) circulation to the liver before entering the blood. Various regulatory mechanisms keep the blood glucose level there constant at around 70 to 80 mg/dl in the long term in healthy individuals. If the glucose level in the enterohepatic circulation increases as a result of a carbohydrate-rich food intake, the beta cells of the pancreas are stimulated to secrete the blood sugar-lowering hormone insulin in order to keep the glucose level in the blood constant. If this regulation fails or the insulin loses its effect, short- or long-term hyperglycemia occurs.
Hyperglycemia is the leading symptom of diabetes mellitus, but is not a definite criterion for it. It can also be triggered by Cushing's disease (increased cortisone levels), acromegaly (increased growth hormone levels), pheochromocytoma (increased levels of adrenaline and noradrenaline), hyperthyroidism (for example as a result of Graves' disease), iron deposits in the beta cells of the pancreas (haemochromatosis) and medication. It can also occur with infections, after a heart attack, stroke or anaesthesia. In bitches, high levels of progesterone in the inter-estrus period can cause a rise in blood glucose levels, and in cats, stress can trigger prolonged hyperglycaemia.
Origin
There are different reasons why the body cannot stabilize the blood glucose level in the physiological range. The most common causes of an increase in blood glucose levels are a reduced response of sugar-storing cells such as fat and muscle cells to insulin (insulin resistance) due to overconsumption of carbohydrates and sugar or a reduced insulin secretion by the pancreas. In the former case, insulin secretion may even be increased. Therefore, the World Health Organization advises a sugar tax to achieve a noticeable decrease in sugar consumption so that fewer people suffer from overweight, obesity and diabetes.
The level of growth hormone (somatropin) is only increased in healthy people when insulin levels are too low. It increases blood sugar levels by both inhibiting the uptake of sugar into fat and muscle cells and reducing sugar consumption by increasing the supply of fats (fatty acid oxidation), particularly in muscle. If both hormones are elevated, hyperglycemia can occur because the blood sugar-lowering effect of insulin on the sugar-storing cells is then limited.
Cortisol increases the blood sugar level. In particular, it stimulates the formation of new sugar in the body and at the same time reduces sugar consumption. Therefore, it counteracts the blood sugar-lowering insulin. If there is an excess of cortisol (Cushing's syndrome, stress), the blood sugar level rises.
Adrenaline and noradrenaline simultaneously lead to increased new formation and release of glucose as well as to an inhibition of insulin secretion. Increased levels, such as those found in pheochromocytoma, lead to hyperglycemia.
In hyperthyroidism glycogenolysis and gluconeogenesis are stimulated, in hemochromatosis the increased iron level in the pancreas leads to siderosis and fibrosis, whereby the function of the insulin-producing beta cells is then also impaired. In glucagonoma, increased glucagon levels cause an increase in gluconeogenesis with a simultaneous decrease in glycogenolysis and glucose consumption.
Serious illnesses such as myocardial infarction, severe infections or trauma can cause hyperglycaemia, as can anaesthesia. The cause is the post-aggression metabolism triggered by this, in which peripheral insulin resistance occurs, whereby the administration of insulin then also does not lead to a sufficient lowering of the blood glucose level. A special case of morning hyperglycemia during ongoing insulin therapy is the Somogyi effect: The Somogyi effect, in which, for example, as a result of excessive evening insulin administration, nocturnal hypoglycemia and subsequent reactive hyperglycemia occur. The Dawn phenomenon is the term used to describe hyperglycaemia that occurs when the increased insulin requirement in the second half of the night is not compensated for as a result of the increased GH excretion at this time, for example as a result of the nocturnal drop in effect of a long-acting insulin after it has been administered once in the morning.

Related articles
Author
AlegsaOnline.com Hyperglycemia — high blood sugar: causes, symptoms, diagnosis, treatment Leandro Alegsa
URL: https://en.alegsaonline.com/art/46159