Hyperkalemia: causes, effects, diagnosis and treatment
Hyperkalemia is an elevated blood potassium level that can impair cardiac conduction. This article covers causes, symptoms, ECG findings, emergency and long‑term management, and notable facts.
Overview
Hyperkalemia refers to an abnormally high concentration of the mineral potassium in the blood. Potassium is essential for normal electrical activity in nerve and muscle cells, especially the heart. When serum potassium rises beyond the normal range it can alter cardiac conduction and, in severe cases, precipitate life‑threatening arrhythmias. Because changes in rhythm may occur suddenly and without preceding symptoms, clinicians treat significant hyperkalemia as a potential medical emergency.
Image gallery
1 Image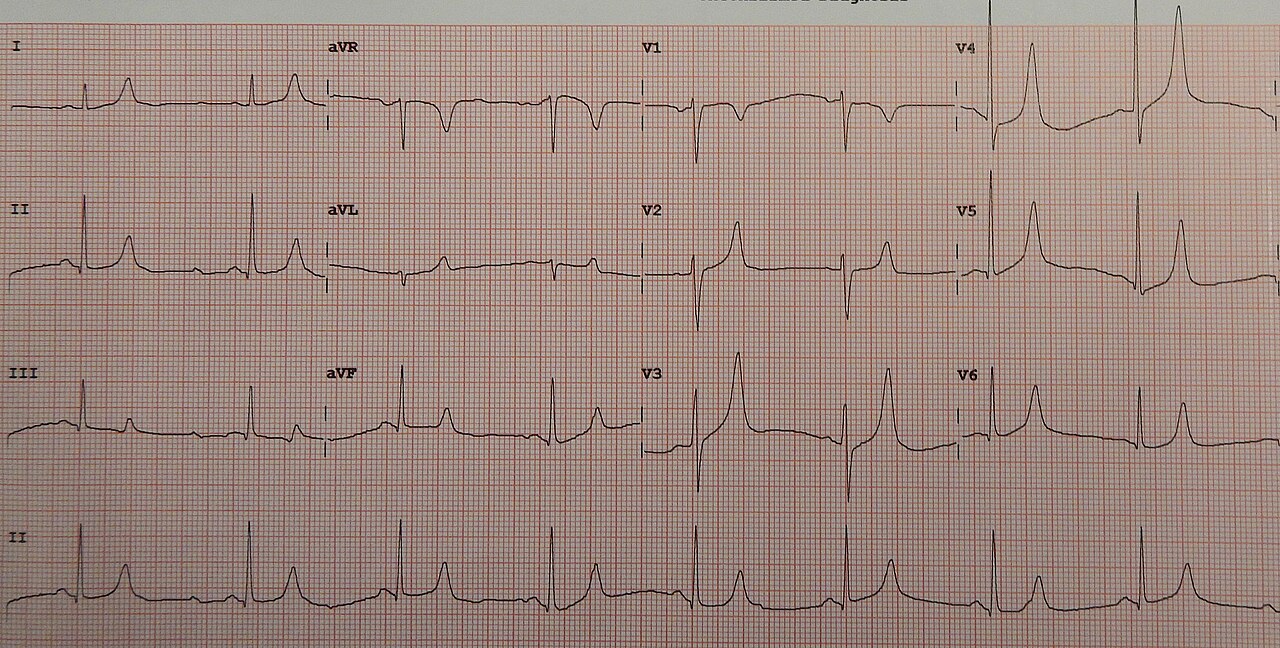
Causes and risk factors
Multiple processes can raise serum potassium by increasing intake, reducing renal excretion, or shifting potassium from cells into the circulation. Underlying impairment of the kidney is the single most important predisposing factor because the kidneys normally remove most excess potassium. Other common contributors include certain medications, tissue breakdown, endocrine disorders, and excessive potassium supplementation.
- Medications: ACE inhibitors, angiotensin receptor blockers, potassium‑sparing diuretics (for example spironolactone), nonsteroidal anti‑inflammatory drugs, some antibiotics and immunosuppressants.
- Reduced excretion: chronic kidney disease or acute kidney injury.
- Cellular release: hemolysis, rhabdomyolysis, severe burns, tumor lysis syndrome.
- Endocrine causes: hypoaldosteronism or adrenal insufficiency and type 4 renal tubular acidosis.
- Excessive intake: oral or intravenous potassium, including some salt substitutes.
Clinical features and diagnosis
Mild elevations may be asymptomatic and discovered incidentally on laboratory testing. Symptoms, when present, can include muscle weakness, paresthesia, nausea, or palpitations. The principal concern is cardiac: hyperkalemia changes the electrocardiogram (ECG) in characteristic ways—tall peaked T waves, loss of P waves, widening of the QRS complex, and, in extreme cases, a sine‑wave pattern—progressing to ventricular fibrillation or asystole if untreated.
Diagnosis relies on serum potassium measurement, assessment of renal function and acid‑base status, and an ECG. Clinicians must also exclude laboratory artifact due to hemolysis of the sample, which can falsely elevate potassium readings.
Management
Treatment of hyperkalemia has two concurrent goals: stabilize the heart and reduce serum potassium. In urgent situations, immediate measures include agents that stabilize cardiac membranes and therapies that shift potassium into cells while definitive removal is arranged.
- Cardiac stabilization: intravenous calcium salts (calcium gluconate or chloride) to reduce the risk of arrhythmia.
- Potassium shifting: insulin with glucose, inhaled beta‑2 agonists, and sodium bicarbonate in selected cases.
- Removal of potassium: loop diuretics if urine output permits, gastrointestinal cation exchangers, newer oral binders, and haemodialysis for severe or refractory cases.
Long‑term measures include adjusting offending medications, treating underlying kidney or endocrine disease, and dietary counseling about potassium intake.
History, notable facts and distinctions
Clinically significant hyperkalemia was recognized as clinicians began correlating blood chemistry with cardiac electrical changes. At the elemental level, potassium was isolated in the early 19th century by Humphry Davy, which later enabled study of its physiological roles. A notable and controversial non‑medical use of potassium is in executions by death penalty protocols: some lethal injections employ mixtures that include potassium salts. For instance, lethal injection cocktails may contain potassium chloride, which raises serum potassium rapidly and can stop the heart.
Because hyperkalemia spans benign, chronic elevations to acute life‑threatening emergencies, evaluation focuses on the degree of elevation, ECG findings, underlying causes, and the tempo of onset. Prompt recognition and appropriate triage are central to preventing fatal outcomes.
Questions and answers
Q: What does hyperkalemia mean?
A: Hyperkalemia is a medical term that indicates that the level of potassium in the blood is too high.
Q: Why is hyperkalemia a medical emergency?
A: Depending on the level of potassium in the blood, hyperkalemia can be a medical emergency because it can lead to abnormal heart rhythms, which can be deadly.
Q: What are the causes of hyperkalemia?
A: Many medications can cause hyperkalemia, and it is much more likely to occur in people with kidney problems.
Q: Does hyperkalemia always cause symptoms?
A: Hyperkalemia often doesn't cause symptoms, but doctors worry about it because it can cause a sudden change of heart rhythm in people who had not been having any symptoms.
Q: What can happen if hyperkalemia causes abnormal heart rhythms?
A: Hyperkalemia can cause abnormal heart rhythms that can be deadly.
Q: Why might hyperkalemia be artificially induced?
A: In cases where death penalty is carried out using lethal injection, a hyperkalemia may be provoked artificially because some of the mixtures used in the injections contain potassium chloride, which will raise the level of potassium in the blood considerably.
Q: What is the danger of inducing hyperkalemia through lethal injection?
A: Inducing hyperkalemia through lethal injection can cause abnormal heart rhythms, which can be deadly.
Related articles
Author
AlegsaOnline.com Hyperkalemia: causes, effects, diagnosis and treatment Leandro Alegsa
URL: https://en.alegsaonline.com/art/46168