Defibrillation: restoring coordinated heart rhythm with an electric shock
Defibrillation is the controlled delivery of an electric shock to stop dangerous heart arrhythmias and permit restoration of a normal heartbeat. Covers mechanisms, devices, uses, and safety.
Overview
Defibrillation is the process of delivering a controlled electric shock to the heart to terminate a life‑threatening arrhythmia and allow the organ's natural pacemaking activity to resume. It is most commonly used for ventricular fibrillation and pulseless ventricular tachycardia, rhythms in which the heart muscle quivers or beats too fast to pump blood effectively. When blood flow to vital organs has ceased, timely defibrillation can be lifesaving; it is often performed alongside cardiopulmonary resuscitation (CPR).
Image gallery
9 Images






How defibrillation works
Defibrillation works by delivering a brief, high‑voltage electric current through the cardiac muscle. The shock depolarizes a critical mass of cardiac cells simultaneously, interrupting the disorganized electrical activity that causes fibrillation. Once the abnormal rhythm is halted, the heart's normal conduction system can reestablish an organized rhythm. This action differs from pacing or low‑energy therapies that gently prompt a heartbeat; defibrillation is an abrupt reset intended for chaotic rhythms.
Types of devices and approaches
- External manual defibrillators are operated by trained clinicians and allow selection of energy and timing.
- Automated external defibrillators (AEDs) analyze rhythm automatically and advise or deliver shocks, designed for use by lay rescuers in public settings.
- Implantable cardioverter‑defibrillators (ICDs) are small devices placed under the skin that continuously monitor heart rhythm and automatically deliver therapy when needed.
- Cardioversion is a related procedure that delivers a synchronized shock to correct some organized but abnormal rhythms; it is distinguished from unsynchronized defibrillation used for chaotic rhythms.
Clinical use and basic procedure
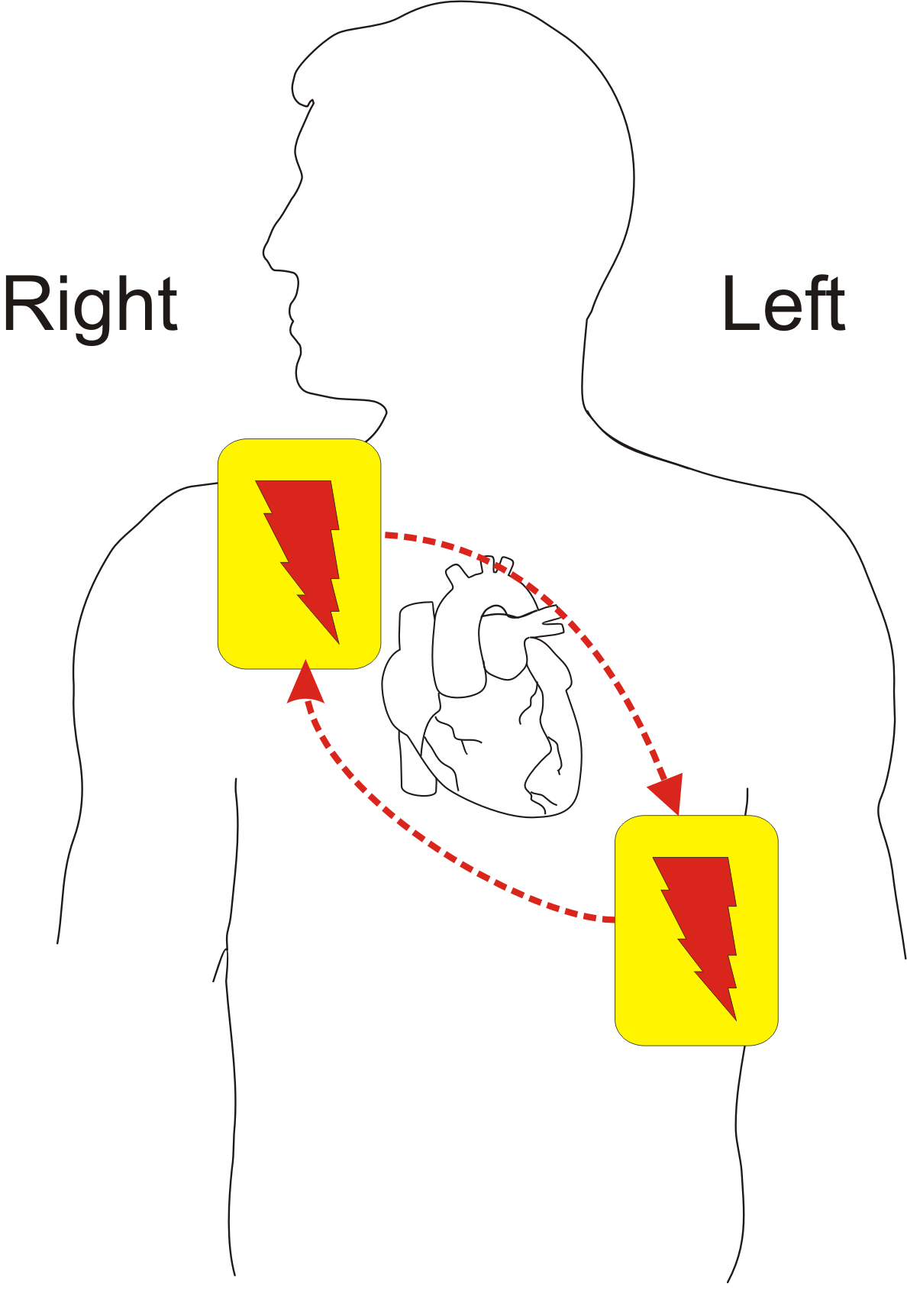
When a patient is found unresponsive and pulseless, rescuers follow a sequence: confirm unresponsiveness and lack of breathing, call for help, begin chest compressions, attach a defibrillator, and follow device prompts. External pads or paddles are placed on the chest to create a conduction path. Many devices give audible instructions and safety prompts to ensure the rescuer and patient are clear before a shock is delivered. Effective CPR before and after shocks improves the chance that defibrillation will restore a sustainable heartbeat.
History and development
Early experiments in the 18th and 19th centuries recognized electrical excitation of muscle; in the 20th century, clinicians developed practical defibrillators for cardiac arrest. Advances include portable units for ambulances and public spaces and the development of automated algorithms and implantable systems. Improvements in waveform design and device intelligence have increased efficacy and safety, enabling broader public access to life‑saving shocks.
Safety, limitations and notable facts
Defibrillation is generally safe when used according to established protocols, but it can cause skin burns beneath pads and may be ineffective if applied too late or if underlying conditions persist. Not all arrhythmias benefit from shock therapy; organized rhythms with a pulse may require different treatments. Training in CPR and AED use significantly improves outcomes. For background reading and device information, see general references on resuscitation and emergency cardiac care, and consult manufacturers or clinical guidelines found via authoritative sources such as professional societies and emergency services (defibrillator resources and heart information).
For practical guidance on recognizing shockable rhythms, device operation, and public access defibrillation programs, search resources that include training courses and local emergency medical service recommendations. Many modern defibrillators combine automated analysis with clear voice prompts to guide rescuers through safe, rapid intervention.
Related articles
Author
AlegsaOnline.com Defibrillation: restoring coordinated heart rhythm with an electric shock Leandro Alegsa
URL: https://en.alegsaonline.com/art/26279
Sources
- heart.org : "Ventricular Fibrillation"
- case.edu : "Claude Beck, defibrillation and CPR"
- ncbi.nlm.nih.gov : "Implantable cardioverter defibrillator"
- prenhall.com : "Defibrillation and Cardiac Arrest"