Defibrillator (AED, ICD): devices for treating life‑threatening heart rhythms
A defibrillator is an electrical device used to stop malignant heart rhythms like ventricular fibrillation and allow the heart's normal rhythm to resume.
Overview
A defibrillator is a medical device that delivers a controlled electric shock to the heart to terminate chaotic electrical activity and restore an organized heartbeat. The treatment is most commonly used for ventricular fibrillation and certain forms of ventricular tachycardia, which can rapidly progress to cardiac arrest if not treated. Defibrillation is a time‑sensitive intervention: the chance of a favorable outcome falls the longer effective therapy is delayed.
Image gallery
9 Images





How it works
The basic goal of defibrillation is to depolarize a critical mass of heart muscle nearly simultaneously so the heart's natural pacemaker can regain coordinated control. The device charges an internal capacitor and releases a brief, high‑current pulse through electrodes placed on the chest. Modern systems use waveforms (commonly biphasic) that improve effectiveness and reduce the energy required compared with earlier designs. The delivered pulse is a form of electrical energy tailored to interrupt disordered rhythms without causing prolonged damage.
Types and components
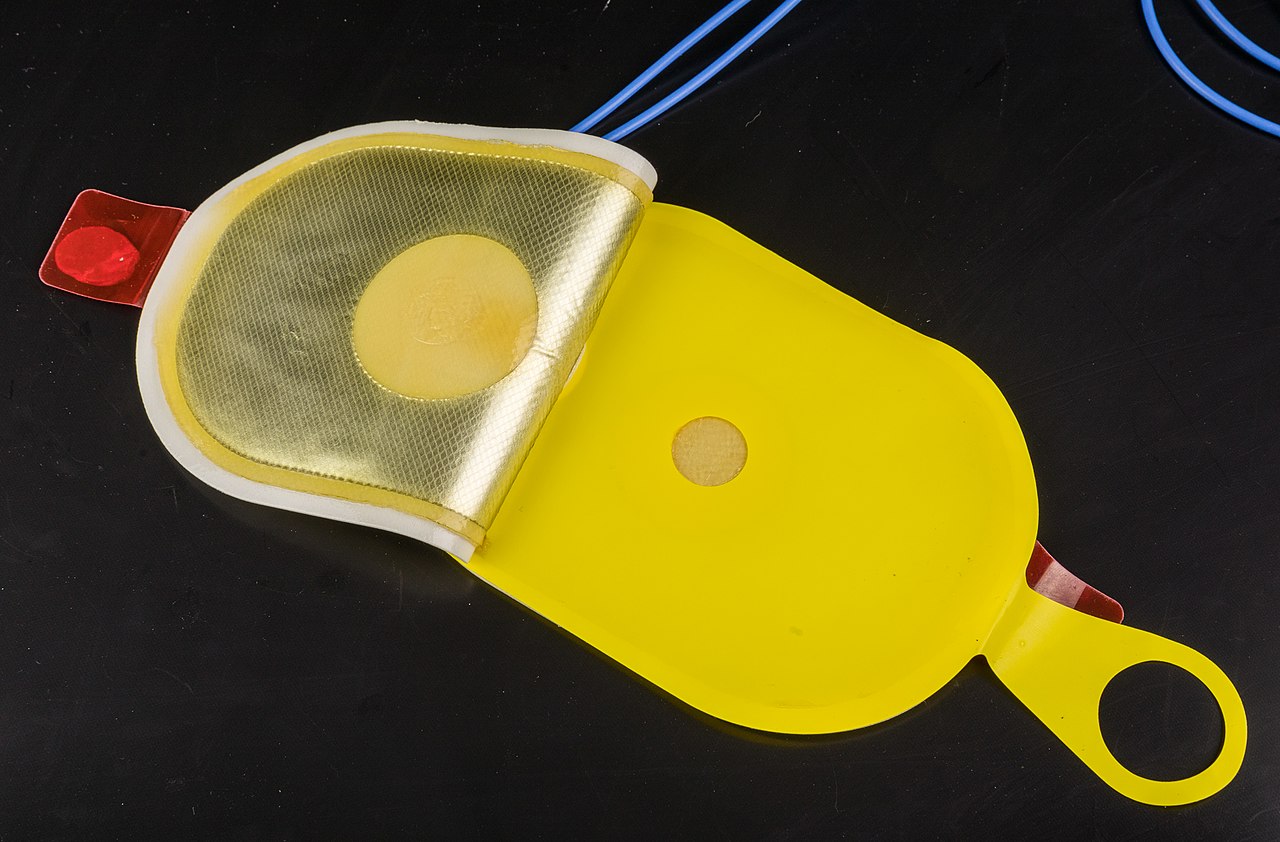
Defibrillators come in several forms and share common components such as a power source, a charging circuit, electrodes (pads or paddles), and control electronics. Major categories include:
- Automated external defibrillators (AEDs) — portable, user‑friendly units with voice prompts and built‑in rhythm analysis so lay rescuers can treat victims quickly.
- Manual defibrillators — used by trained clinicians who interpret the rhythm and select the energy and timing for shocks.
- Implantable cardioverter‑defibrillators (ICDs) — surgically placed devices that continuously monitor the heart and deliver internal shocks when dangerous rhythms are detected.
When and how it is used
Defibrillation is indicated for specific shockable arrhythmias, most notably ventricular fibrillation and pulseless ventricular tachycardia. In emergency care, it is integrated with basic and advanced life support measures: high‑quality cardiopulmonary resuscitation (CPR) maintains some circulation until a shock can be delivered, and post‑shock care supports recovery. For AED use, rescuers follow on‑screen and audible instructions; when using manual devices, clinicians synchronize shocks for certain rhythms or select unsynchronized shocks for fibrillation.
History and significance
Defibrillators evolved through the 20th century as electrical and biomedical engineering advanced. Early devices were large and required expert operation; later innovations made them faster, safer, and widely accessible. Public access to AEDs in airports, schools, and workplaces has become an important public health measure because rapid defibrillation markedly improves survival from sudden cardiac arrest when combined with bystander CPR.
Limitations and safety
Defibrillation does not guarantee restoration of a normal rhythm and is not appropriate for all cardiac arrests (for example, asystole or pulseless electrical activity are generally non‑shockable). Safety precautions include ensuring no one touches the patient during shock delivery and avoiding conductive surfaces. Successful outcomes depend on prompt recognition, rapid access to a defibrillator, effective CPR, and advanced medical care afterward. For further technical or clinical details see authoritative resources at ventricular fibrillation information and equipment guidance at energy and waveform references.
Questions and answers
Q: What is a defibrillator?
A: A defibrillator is a machine that is used when ventricular fibrillation happens in the heart of a human.
Q: What is the purpose of a defibrillator?
A: The purpose of a defibrillator is to save a person's life by correcting ventricular fibrillation.
Q: What happens during ventricular fibrillation?
A: During ventricular fibrillation, many different cells in the heart begin to act as pacemaker cells, causing confusion and an inability to move blood around the body.
Q: How does a defibrillator work?
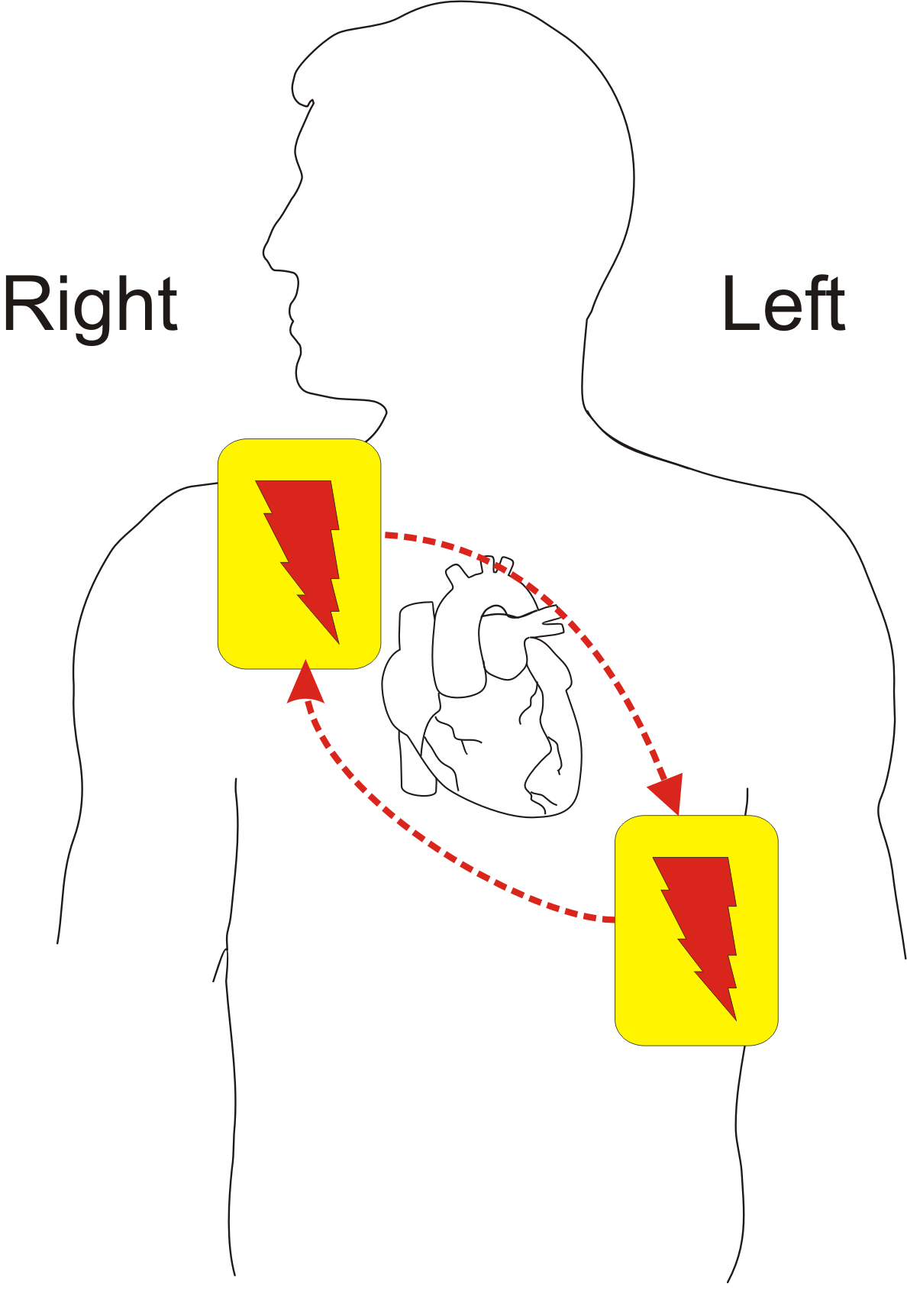
A: A defibrillator sends a high energy pulse from the top-right of the heart to the bottom-middle of the heart, causing the whole heart to stop all activity. This allows the heart's normal pacemaker to restart normal beating.
Q: Is defibrillation always successful?
A: No, defibrillation does not always work.
Q: Why is defibrillation important?
A: Defibrillation is important because it can save a person's life when experiencing ventricular fibrillation, which can lead to cardiac arrest and death.
Q: What is the main cause of ventricular fibrillation?
A: The main cause of ventricular fibrillation is when many different cells in the heart act as pacemaker cells, causing confusion and an inability to move blood around the body.
Related articles
Author
AlegsaOnline.com Defibrillator (AED, ICD): devices for treating life‑threatening heart rhythms Leandro Alegsa
URL: https://en.alegsaonline.com/art/26280