Cataplexy: sudden emotion‑triggered muscle weakness
Cataplexy is a sudden, brief loss of voluntary muscle control often brought on by strong emotions. Linked with narcolepsy, it is diagnosed clinically and managed with medication and safety strategies.
Overview
Cataplexy is a neurological symptom characterized by abrupt, transient loss of muscle tone that is usually provoked by strong emotions such as laughter, surprise, anger or fear. During an episode a person remains conscious and aware but experiences partial or complete weakness of muscles — for example, drooping of the eyelids, buckling knees, slurred speech, or total collapse. Episodes typically last seconds to a few minutes and resolve without aftereffects, though repeated events can injure the person if precautions are not taken.
Image gallery
2 Images
Causes and mechanism
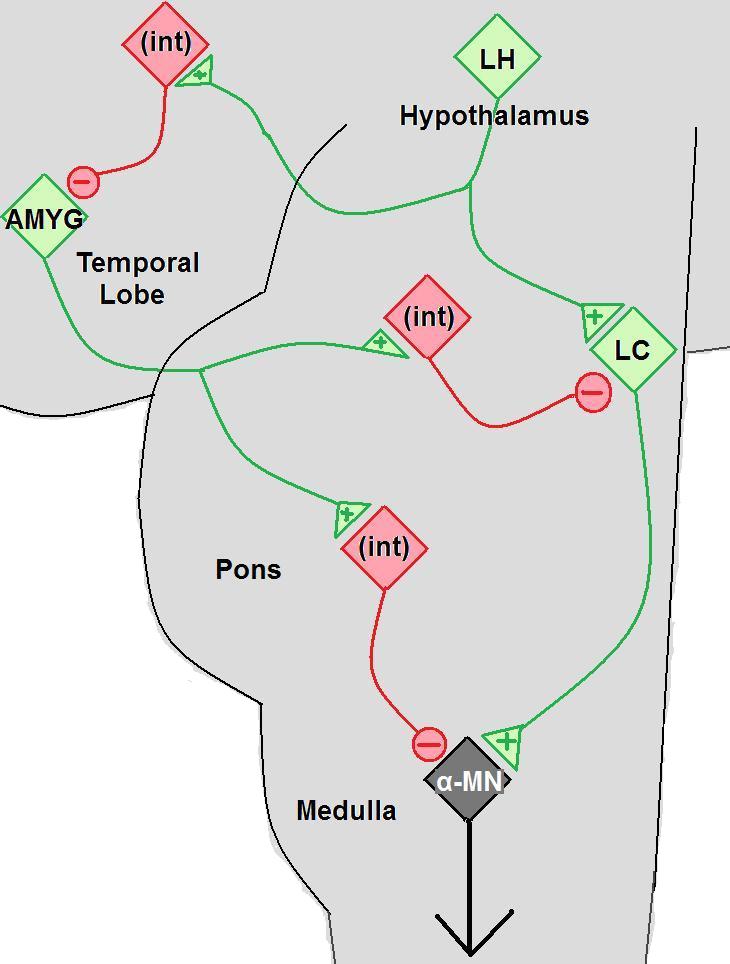
Cataplexy is most commonly associated with narcolepsy, especially the subtype linked to loss of hypocretin (also called orexin) producing neurons in the brain. The prevailing explanation is that elements of REM sleep physiology — specifically the neural circuits that produce muscle atonia — intrude into wakefulness. Emotional triggers appear to activate pathways that normally coordinate muscle suppression during REM sleep, producing abrupt weakness while awareness is preserved.
Typical features and diagnosis
Recognizing cataplexy depends largely on clinical history. Key features include preserved consciousness during episodes, clear emotional precipitants, and rapid recovery. Affected muscle groups vary and can be focal or generalized. Physicians often ask detailed eyewitness descriptions and may use sleep studies such as nocturnal polysomnography and the multiple sleep latency test to assess for narcolepsy. Cerebrospinal fluid testing for hypocretin can be informative in selected cases.
Management and practical measures
Treatment aims to reduce the frequency and severity of episodes and to improve safety and quality of life. Options include medications that suppress REM-related muscle atonia (for example, certain antidepressants) and agents that consolidate sleep and reduce daytime sleepiness, such as sodium oxybate in regulated settings. Behavioral measures — avoiding known emotional triggers when possible, arranging safe environments to prevent injury during sudden falls, and educating family or coworkers — are important adjuncts.
Distinctive points and differential diagnosis
Cataplexy differs from seizures and fainting in several ways: consciousness is maintained, episodes are brief and emotion-linked, and there is no abnormal electrical activity on EEG caused by cataplexy itself. For clarity, consult differential lists that include epilepsy, syncope and functional neurological disorders. When muscles fail in isolation it may be useful to reference normal motor anatomy such as muscles and their control pathways.
History, terminology and further reading
The word cataplexy comes from Greek roots meaning "down" and "stroke or seizure," reflecting the sudden loss of tone. Because of its frequent association with narcolepsy, cataplexy is discussed in sleep medicine and neurology texts; readers seeking clinical guidance can consult specialist resources. For basic definitions and distinctions related to seizures or similar events see discussions of seizures and reviews of the Greek etymology at classical language sources.
- Key signs: emotion-triggered weakness, preserved awareness, brief duration.
- When to seek care: frequent episodes, injury risk, or accompanying excessive daytime sleepiness.
- Important tests: clinical history, sleep studies, and selective biochemical assays.
Related articles
Author
AlegsaOnline.com Cataplexy: sudden emotion‑triggered muscle weakness Leandro Alegsa
URL: https://en.alegsaonline.com/art/17585