Kaposi's sarcoma: causes, forms, signs, diagnosis and treatment
Kaposi's sarcoma is a tumor linked to human herpesvirus 8 (HHV‑8) that produces purple skin and internal lesions. Overview of types, clinical features, diagnosis, therapy, and historical notes.
Kaposi's sarcoma is a vascular tumor that most often appears as purple, red or brown patches, plaques, or nodules on the skin and mucous membranes. It can also involve lymph nodes and internal organs. The condition is associated with infection by human herpesvirus 8 (HHV‑8) and is most likely to develop when the immune system is weakened.
Image gallery
9 Images







Cause and biology
The driving factor is HHV‑8, a virus that infects endothelial and related cells and can promote abnormal blood vessel growth. Immune suppression—whether from HIV infection, immunosuppressive drugs after organ transplantation, or other causes—greatly increases the risk that infected cells will form visible lesions. Not every person with HHV‑8 develops the disease; host factors and immune status influence progression.
Clinical forms
- Classic: typically slow-growing lesions on the lower legs of older adults, more common in people of Mediterranean or eastern European descent.
- Endemic (African): occurs in parts of Africa and may affect younger people and children, sometimes with more aggressive behavior.
- Epidemic (AIDS‑associated): linked to HIV infection and was a common complication early in the AIDS epidemic; lesions can be widespread and involve internal organs.
- Iatrogenic (transplant-associated): appears in people receiving immunosuppressive therapy after organ transplantation; reducing immune suppression can lead to improvement.
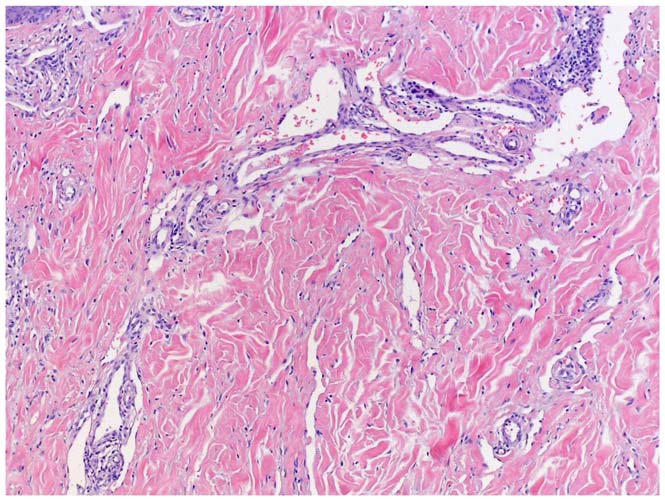
Presentation and diagnosis
Skin lesions vary from flat patches to raised nodules and are often described as purple or reddish. Lesions may be painless but can ulcerate, bleed, or cause swelling if they involve lymphatic channels. Mucosal and visceral involvement (lungs, gastrointestinal tract) can produce cough, bleeding, or organ-specific symptoms. Evaluation typically includes clinical examination, biopsy for histopathology and immunohistochemistry, and tests to assess immune status and extent of internal disease. See general background on the condition at Kaposi's sarcoma overview and information on typical skin changes at skin lesions.
Treatment and prognosis
Management depends on type, extent, and patient health. In HIV‑associated cases, effective antiretroviral therapy often leads to regression. Local measures—surgical excision, cryotherapy, laser, or radiation—are used for limited skin disease. Systemic therapies, including chemotherapy or immunomodulatory agents, are reserved for extensive or visceral involvement. Prognosis varies: some cases remain indolent for years while others progress more rapidly, particularly when immune control is poor.
Historically described by Moritz Kaposi in the 19th century, the disease gained broader public attention with the rise of the HIV epidemic. Public health efforts that reduce immunosuppression and manage HHV‑8 exposure help limit disease burden. Ongoing research seeks better targeted therapies and strategies to prevent HHV‑8 transmission.
Related articles
Author
AlegsaOnline.com Kaposi's sarcoma: causes, forms, signs, diagnosis and treatment Leandro Alegsa
URL: https://en.alegsaonline.com/art/52234
Sources
- ncbi.nlm.nih.gov : "Cutaneous lesions of the nose"
- doi.org : 10.1186/1746-160X-6-7
- pubmed.ncbi.nlm.nih.gov : 20525327
- thefreedictionary.com : thefreedictionary.com/Kaposi's sarcoma
- cancer.gov : "Kaposi Sarcoma Treatment"
- ncbi.nlm.nih.gov : "Diagnosis and Treatment of Kaposi Sarcoma"
- doi.org : 10.1007/s40257-017-0270-4
- pubmed.ncbi.nlm.nih.gov : 28324233
- doi.org : 10.1016/j.jaad.2008.05.001
- pubmed.ncbi.nlm.nih.gov : 18638627
- gco.iarc.fr : "Kaposi sarcoma"