Anterior cruciate ligament (ACL)
The anterior cruciate ligament (ACL) is a major knee ligament that stabilizes the joint. Tears occur often in pivoting sports and are managed with rehabilitation or surgical reconstruction plus months of physiotherapy.
Overview
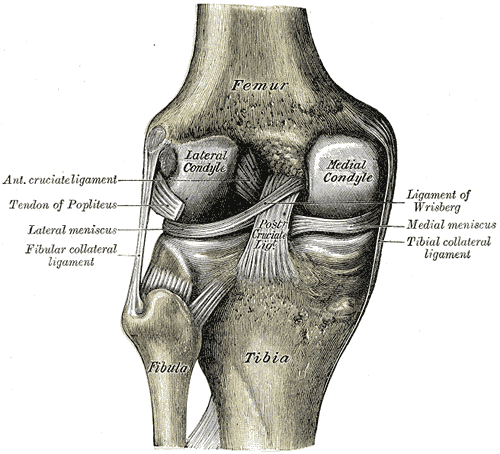
The anterior cruciate ligament, commonly abbreviated ACL, is one of the four major ligaments that stabilize the human knee. It runs diagonally through the center of the knee and connects the femur (thigh bone) to the tibia (shin bone). Its primary roles are to resist forward translation of the tibia relative to the femur and to control rotational stability during cutting, pivoting, and landing movements.
Image gallery
7 Images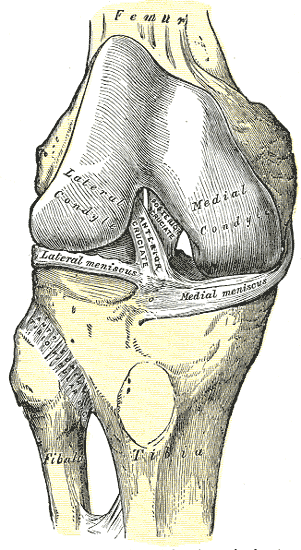





Anatomy and function
The ACL consists of two bundles that tighten at different angles of knee flexion, allowing dynamic control across the joint's range of motion. It works together with the posterior cruciate ligament (PCL) and the collateral ligaments to maintain mechanical stability and coordinate normal gait and sports movements. Damage to the ACL compromises this balance and often produces a sensation of instability or "giving way."
Injury mechanisms and risk factors
ACL injuries commonly occur when the foot is planted and the body changes direction, when landing from a jump, or during direct contact to the knee. Non-contact injuries are frequent in sports that require sudden deceleration and pivoting, such as soccer, basketball, American football and skiing. Many athletes are affected, and research has shown sex, neuromuscular control, footwear, playing surface and prior injury history are among factors that influence risk.
Signs, diagnosis and examples
Typical immediate signs include a sharp pain, rapid swelling, and often an audible "pop." Patients may report instability with weight bearing. Diagnosis is made by clinical examination (Lachman, pivot-shift tests) and confirmed with imaging such as magnetic resonance imaging (MRI). Early assessment helps guide treatment decisions and rehabilitation planning.
Treatment options and recovery
Management ranges from structured non-surgical rehabilitation to surgical reconstruction. Isolated partial tears or less active individuals may do well with physical therapy focused on strength and neuromuscular training. Complete ruptures in active patients are frequently treated with ACL reconstruction, which replaces the torn ligament with a graft (autograft or allograft) and is followed by progressive rehabilitation over several months. Decisions about surgery should be individualized and discussed with an orthopedic specialist; in many cases, operative restoration of stability is chosen to allow return to pivoting sports and reduce further joint damage from recurrent instability. See also: surgical options.
Prevention, prognosis and notable facts
Prevention programs that teach landing technique, balance, and strength have reduced ACL injury rates in some populations. Although many patients return to high-level activity after treatment, an ACL tear is associated with a long-term increased risk of knee osteoarthritis. Female athletes show a higher incidence of ACL injury in several sports, and this difference has prompted targeted prevention research. For detailed rehabilitation protocols and surgical considerations consult specialist resources and clinicians.
- Common symptoms: pain, swelling, instability, difficulty bearing weight.
- Typical causes: pivoting, sudden deceleration, awkward landings, contact to the knee.
- Key prevention: neuromuscular training, strength and technique coaching.
For more clinical guidance and patient information, refer to specialist orthopedic materials and trusted professional guidelines available from sports medicine and joint health organizations.
Major knee ligaments • Knee joint anatomy • Athletes and ACL risk • Surgical reconstruction
Related articles
Author
AlegsaOnline.com Anterior cruciate ligament (ACL) Leandro Alegsa
URL: https://en.alegsaonline.com/art/4563