Eczema: causes, types, symptoms, and management
Eczema is a common inflammatory skin condition causing dry, itchy, red patches. This article explains its types, causes, diagnosis, treatments, and practical self-care measures.
Eczema, also called dermatitis, is a group of conditions in which the outer layer of the skin becomes inflamed, dry and itchy. The word eczema derives from the Greek for "to boil over," reflecting the red, often scaly or oozing appearance of affected skin. Eczema is a clinical diagnosis, and it is not contagious. It arises where the dermatitis process affects the epidermis and is driven by a mix of skin barrier weakness and immune activity rather than by infection alone. The term describes a pattern of symptoms rather than a single single disease entity, and it can range from episodic mild flares to persistent, severe disease that impairs sleep and quality of life.
Image gallery
7 Images




Common signs and where it appears
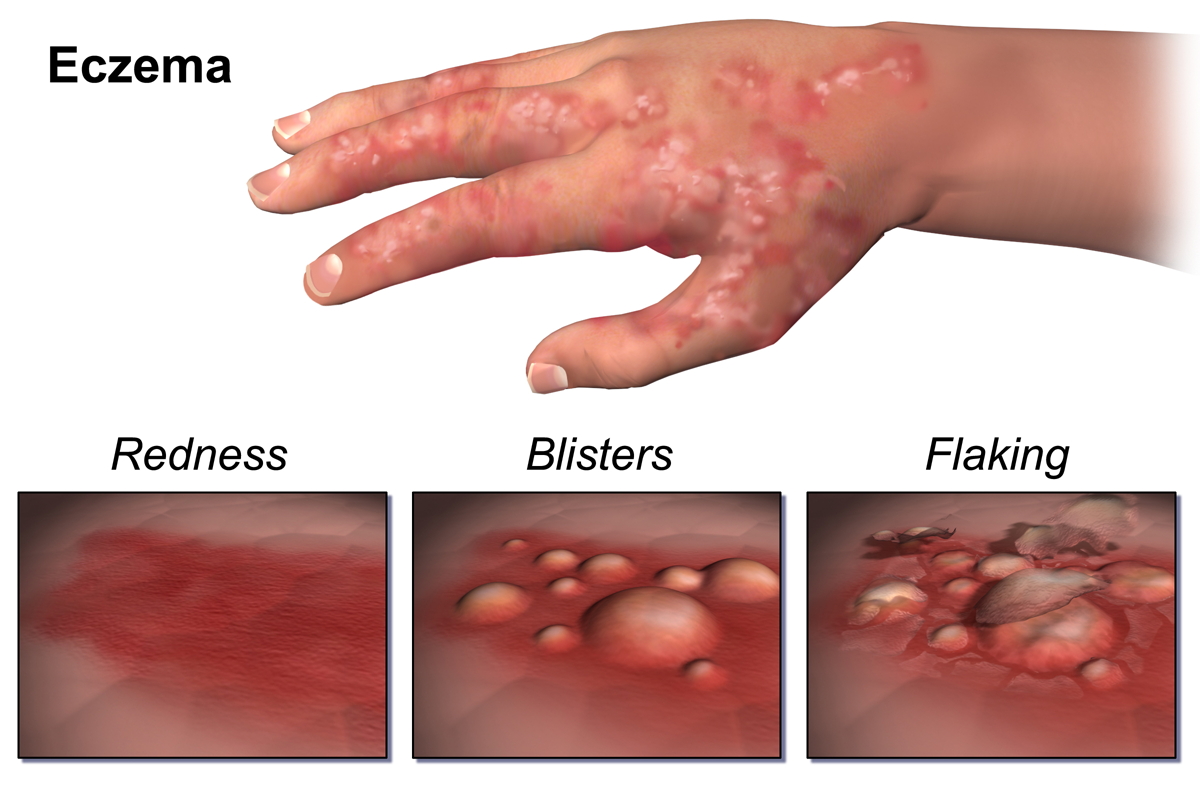
Typical features include intense itching, dry or cracked skin, red or pink patches, small blisters that may weep or crust, and thickened areas from chronic rubbing (lichenification). In infants, eczema often begins on the cheeks and scalp and may later involve the trunk and the creases of limbs. In older children and adults it frequently affects the flexural areas—behind the knees, inside the elbows, around the wrists, neck and hands—and may appear on the eyelids and feet. Episodes can be provoked or worsened by extremes of temperature, sweating, rapid changes in humidity, friction and certain irritants or allergens.
Types and notable variants
- Atopic dermatitis: the commonest form, often starting in childhood and linked to a family history of eczema, asthma or hay fever.
- Contact dermatitis: occurs after the skin touches an irritant (irritant contact) or an allergen (allergic contact); identifying and avoiding the trigger is key.
- Dyshidrotic eczema: small, itchy blisters on the hands and feet.
- Nummular eczema: coin-shaped patches of irritated skin.
- Neurodermatitis: localized, thickened plaques caused by repetitive scratching or rubbing.
Causes and underlying mechanisms
Several factors interact to produce eczema. A primary defect in the skin barrier is common: when the outer layers do not retain moisture effectively, the skin becomes vulnerable to irritants, allergens and microbes. Genetic predisposition plays an important role; family history of atopy increases risk and certain gene variations involved in skin structure and immunity have been associated with the condition. Environmental contributors include dry air, harsh soaps, fragrances, wool or synthetic fabrics, and exposure to allergens such as dust mites, pet dander or certain foods in some children. Psychological stress and infections can trigger or amplify flares. The visible inflammation reflects a complex immune response rather than simple surface irritation.
Diagnosis and important distinctions
Diagnosis is usually clinical, based on appearance, distribution and history. Tests such as patch testing can help identify contact allergens, while blood tests are not routinely required. Differentiating eczema from other chronic rashes—such as psoriasis, fungal infections or scabies—is important because treatments and avoidance strategies differ. Unlike fungal infections or scabies, eczema is not infectious and cannot be passed from person to person. Reliable resources on skin anatomy and inflammation can clarify these distinctions; see general references on inflammation and the structure of the skin.
Treatment and everyday management
Management aims to restore the skin barrier, reduce inflammation, control itching and avoid triggers. Key measures include:
- Regular use of emollients (moisturizers) to hydrate and protect the skin; apply liberally and often, especially after bathing.
- Topical anti-inflammatory treatments: low- to mid-potency topical corticosteroids for flares, and non-steroidal options (topical calcineurin inhibitors) for sensitive areas or long-term use under guidance.
- Antihistamines may help reduce itch and improve sleep for some patients; sedating antihistamines such as hydroxyzine are sometimes used at night for severe itch.
- For persistent moderate-to-severe disease, phototherapy or systemic therapies (immunosuppressants) can be considered under specialist care. Biologic medicines that target specific immune pathways (for example, injections given every few weeks) offer another option for selected patients who do not respond to standard treatments.
- Short courses of oral antibiotics or topical antiseptics may be needed when secondary bacterial infection develops.
- Practical skin care: use lukewarm baths, avoid harsh soaps and rubbing, wear soft cotton clothing, and protect hands with gloves when using detergents.
Prognosis and impact
Eczema often begins in childhood and many people experience improvement with age, but some remain affected into adulthood. Severity varies and the condition can cause significant discomfort, disrupted sleep and emotional distress. With appropriate education, trigger reduction, and a combination of topical and, when necessary, systemic therapies, most people can achieve good control of symptoms. Long-term follow-up and adjustment of the treatment plan help maintain skin health and quality of life.
For more detailed clinical guidance or resources on managing specific triggers and therapies, consult specialist dermatology sources or clinical guidelines. Additional reading on related concepts can be found at linked entries for dermatitis, inflammation, the epidermis and skin.
Related articles
Author
AlegsaOnline.com Eczema: causes, types, symptoms, and management Leandro Alegsa
URL: https://en.alegsaonline.com/art/30008