Cystitis: causes, symptoms, diagnosis, treatment and prevention
Cystitis is inflammation or infection of the urinary bladder. This article explains common causes, symptoms, diagnosis, treatment options, prevention measures, and important distinctions.
Overview
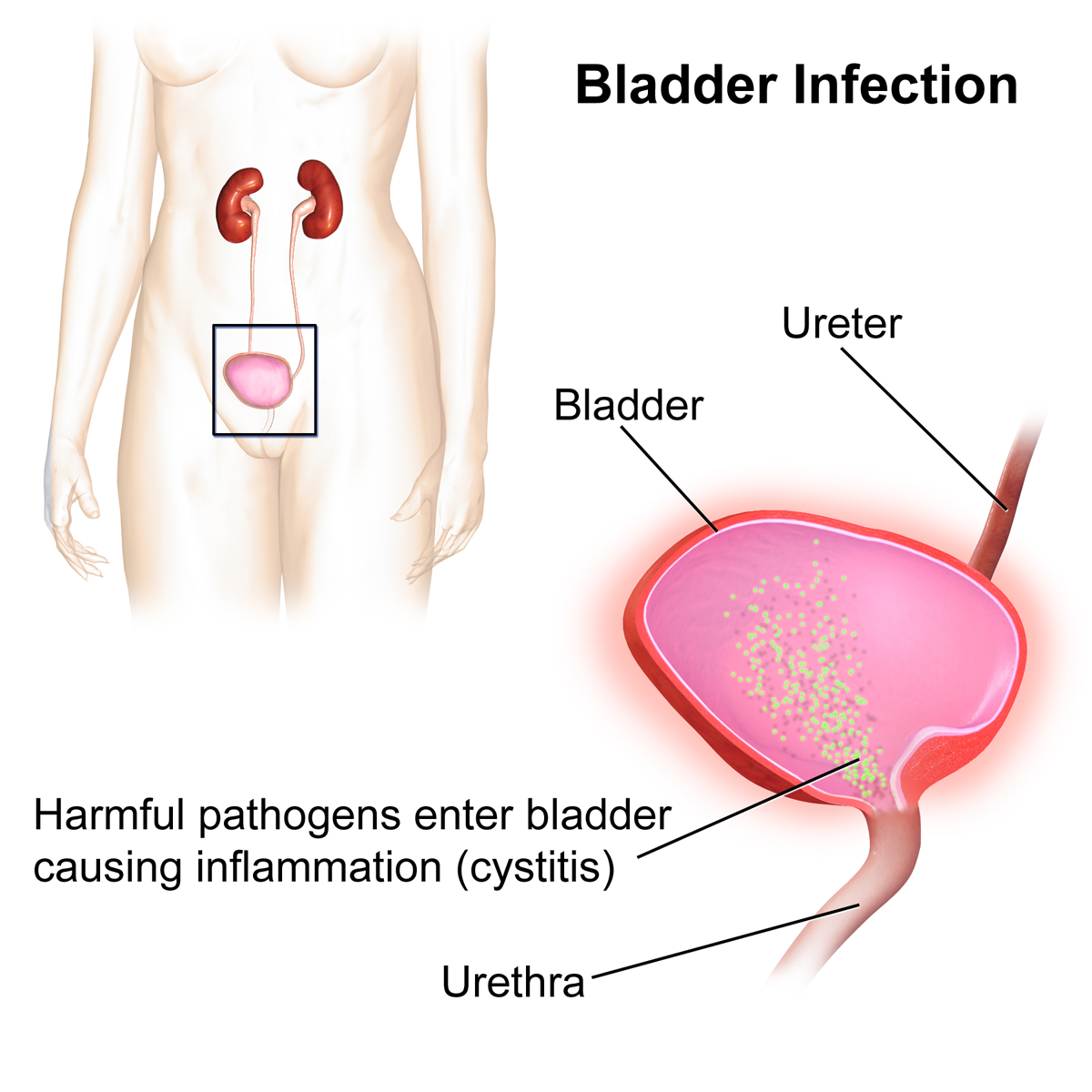
Cystitis is inflammation of the urinary bladder, most commonly caused by a bacterial infection. It can affect people of any age and sex but is far more frequent in women because their urethra is shorter and closer to the anus. Episodes range from a single acute infection to recurrent or chronic irritation; non‑infectious forms also occur.
Image gallery
6 Images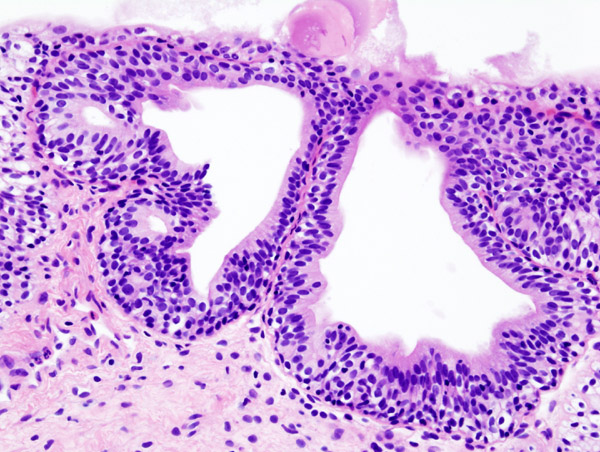




Causes and mechanisms
The usual mechanism is ascent of microbes from the urethral opening into the bladder. Escherichia coli, which normally lives in the gut, is the most common bacterial cause. Other risk factors include sexual activity, catheter use, anatomical abnormalities, reduced immune function, pregnancy and some metabolic conditions. Some cases are inflammatory rather than infectious, as in interstitial cystitis (painful bladder syndrome).
Symptoms and clinical features
- Frequent urination and sudden urgency
- Painful or burning urination (dysuria)
- Lower abdominal discomfort or pressure
- Cloudy or foul‑smelling urine; sometimes visible blood (hematuria)
- Fever is uncommon with simple bladder infection and suggests a higher or systemic infection
Diagnosis and classification
Diagnosis usually relies on history and urinalysis; a urine culture can identify the organism and antibiotic sensitivities when needed. Clinicians distinguish uncomplicated cystitis (typical, otherwise healthy patients) from complicated cystitis (associated with structural, functional, or systemic risk factors). Recurrent cystitis and interstitial cystitis are managed differently from isolated acute infections.
Treatment and prevention
Uncomplicated bacterial cystitis is often treated with a short course of appropriate antibiotics, symptom relief (pain control, hydration) and advice on preventive measures. Preventive strategies include good genital hygiene, adequate fluid intake, voiding after intercourse, careful catheter care and management of underlying conditions. Asymptomatic bacteriuria is usually not treated except in pregnancy or before some urological procedures.
Importance and notable facts
Left untreated or in vulnerable patients, bladder infection can ascend to the kidneys (pyelonephritis) or contribute to sepsis. Rising antibiotic resistance makes accurate diagnosis and prudent antibiotic use important. For detailed clinical guidance and patient resources see clinical information and official recommendations; research into non‑infectious bladder pain syndromes and new prevention strategies is ongoing.
Related articles
Author
AlegsaOnline.com Cystitis: causes, symptoms, diagnosis, treatment and prevention Leandro Alegsa
URL: https://en.alegsaonline.com/art/24953