Carpals (Wrist Bones): Structure, Function, and Clinical Notes
The carpals are eight small bones that form the wrist. This entry summarizes their arrangement, articulations, function, development, common injuries, and useful clinical mnemonics.
Overview
The carpals are eight irregular bones that form the carpus, commonly called the wrist. They connect the forearm to the hand, provide a stable but flexible platform for hand movements, transmit forces from the hand to the forearm, and serve as attachment sites for ligaments and tendons.
Image gallery
7 Images





Anatomy and arrangement
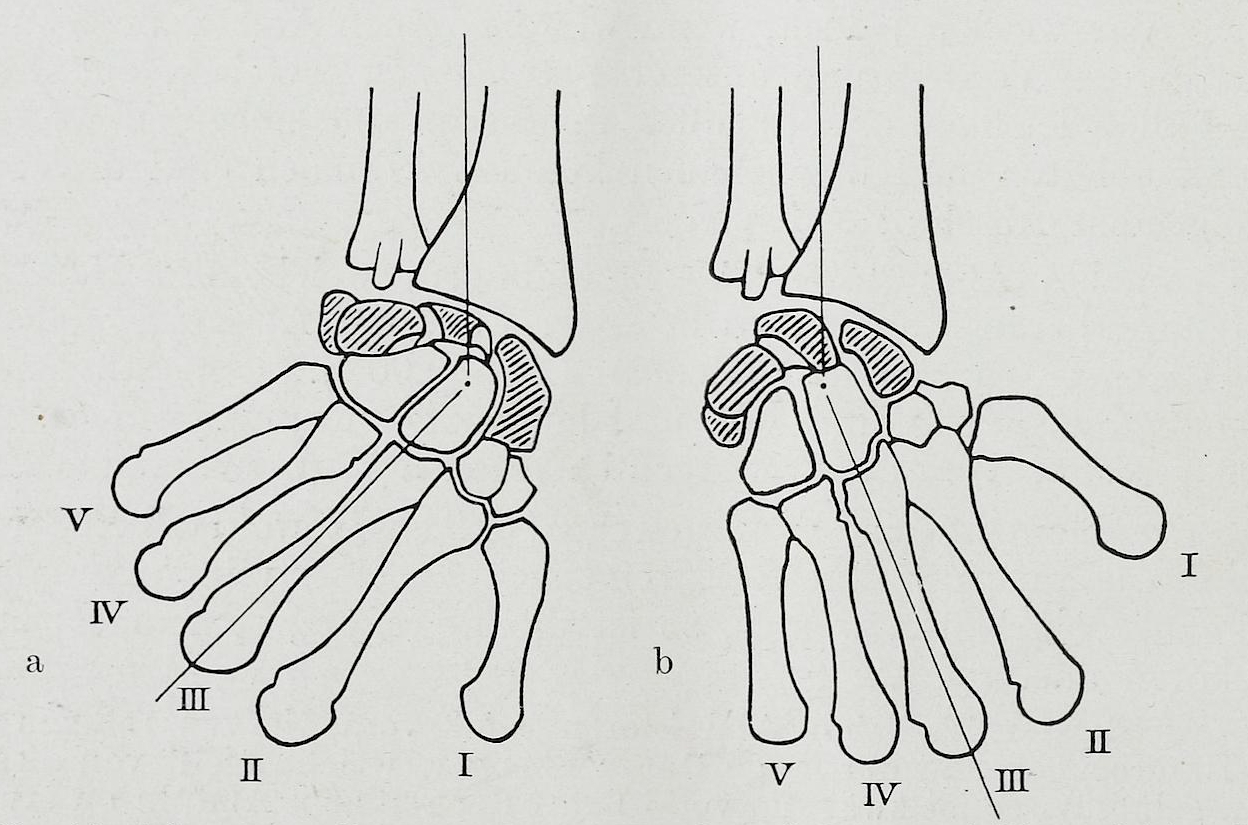
The carpals are arranged in two transverse rows across the wrist. From the radial (thumb) side toward the ulnar (little finger) side they are conventionally listed as:
- Proximal row: Scaphoid, Lunate, Triquetrum, Pisiform.
- Distal row: Trapezium, Trapezoid, Capitate, Hamate.
The scaphoid and lunate articulate with the radius to form the main radiocarpal joint. The pisiform is a sesamoid bone embedded in the tendon of the flexor carpi ulnaris. The capitate is the largest central carpal and acts as a keystone in carpal alignment; the hamate is notable for its palmar hook (hamulus).
Articulations and ligaments
Carpal bones articulate with one another, with the radius and ulna, and with the bases of the metacarpal bones. Intercarpal ligaments and the complex of intrinsic and extrinsic ligaments maintain stability. The scapholunate ligament is especially important: its injury can lead to instability and altered wrist mechanics. The transverse carpal ligament forms the roof of the carpal tunnel, with the carpal bones forming the floor.
Function and biomechanics
The arrangement of the carpals allows flexion, extension, radial and ulnar deviation, and contributes to grip strength and dexterity. The proximal row tends to be more mobile and conforms to movements of the distal radius, while the distal row is more rigid and transmits loads to the metacarpals. Coordinated motion across the rows permits smooth wrist movement and load distribution.
Clinical significance
Several clinical conditions commonly affect the carpals. Scaphoid fractures are frequent after a fall on an outstretched hand and can be difficult to detect on initial radiographs; they are susceptible to impaired healing because of their blood supply. Lunate dislocation or compression can cause acute pain and median nerve symptoms; chronic loss of lunate vascularity is known as Kienböck’s disease. Carpal tunnel syndrome results from compression of the median nerve beneath the transverse carpal ligament. Other issues include osteoarthritis of the wrist, fractures of the hamate or its hook (often sports-related), and ossicle or fusion variants that may be asymptomatic or cause pain.
Investigation and management
Plain radiographs are the initial imaging modality for suspected carpal injury. When radiographs are inconclusive but clinical suspicion remains, MRI or CT can detect occult fractures, ligament tears, or avascular changes. Treatment depends on the injury: many stable fractures and mild sprains are managed conservatively with immobilization and rehabilitation, while displaced fractures, unstable ligament injuries, or chronic compressive neuropathies often require surgical intervention such as fixation, ligament repair, or carpal tunnel release.
Development and variation
Carpal bones develop from cartilaginous precursors and ossify at different times during childhood and adolescence. Anatomical variation is relatively common: the pisiform is a sesamoid, and accessory ossicles or partial fusions between carpals may be present without causing symptoms. Knowledge of typical variants helps avoid misinterpretation of imaging studies.
Memory aids and notable facts
A frequently used mnemonic to recall the carpal sequence from radial to ulnar is: "Some Lovers Try Positions That They Can't Handle" (Scaphoid, Lunate, Triquetrum, Pisiform, Trapezium, Trapezoid, Capitate, Hamate). Understanding carpal anatomy is essential for diagnosing wrist injuries, planning surgery, and interpreting wrist imaging.
Related articles
Author
AlegsaOnline.com Carpals (Wrist Bones): Structure, Function, and Clinical Notes Leandro Alegsa
URL: https://en.alegsaonline.com/art/17221