Squamous cell carcinoma
A group of cancers that arise from squamous epithelial cells in skin and mucous membranes; includes cutaneous and mucosal types with varied causes, presentations, and treatments.
Overview
Squamous cell carcinoma (SCC), sometimes called epidermoid carcinoma, denotes a set of malignant tumours that develop from squamous epithelial cells. These flat, scale‑like cells form the outer layer of skin and line many hollow organs and passages. SCCs occur in the skin and in mucosal surfaces such as the mouth, throat, larynx, esophagus, cervix, anus and portions of the lung and urinary tract. Different clinical subtypes and behaviours exist depending on the organ involved; see the list below for common examples.
Image gallery
10 Images








Common sites and types
- Cutaneous SCC: arises on sun‑exposed skin and is one of the most frequent skin cancers.
- Head and neck SCC: includes cancers of the oral cavity, pharynx and larynx; often linked to tobacco, alcohol and human papillomavirus (HPV).
- Esophageal and pulmonary SCC: tumours of the oesophagus and central airways with distinct risk factors and management.
- Gynecologic and anogenital SCCs: cervical and anal SCC are strongly associated with high‑risk HPV infection.
Pathology and diagnosis
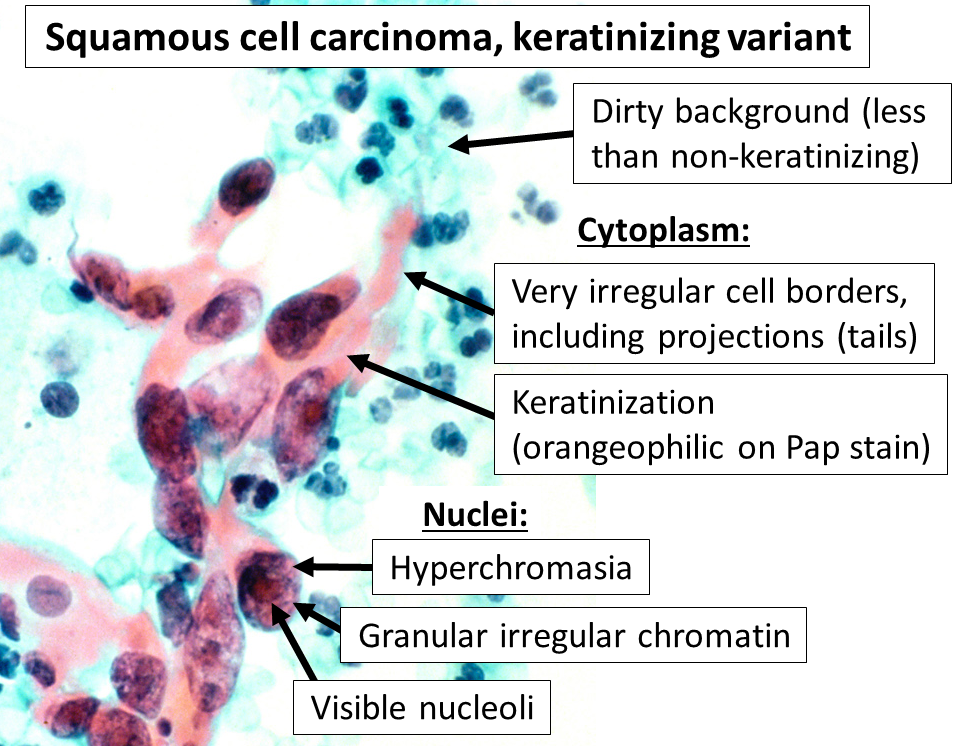
Diagnosis relies on tissue biopsy and microscopic examination. Characteristic histologic features include keratinisation, keratin pearls and intercellular bridges in well‑differentiated tumours; poorly differentiated lesions lose these features. Staging follows established clinical and imaging protocols for the organ involved. Biopsy also guides treatment decisions and prognostic estimates.
Causes and risk factors
Key contributors vary by site but commonly include ultraviolet (UV) radiation for skin SCC, tobacco and alcohol for head and neck and lung SCCs, chronic irritation or inflammation, certain chemical exposures, immunosuppression, and oncogenic viruses such as HPV. Prevention strategies therefore combine sun protection, tobacco cessation and HPV vaccination when appropriate.
Treatment and prognosis
Management depends on stage, location and patient factors. Localised cutaneous SCCs are often treated with surgical excision or Mohs micrographic surgery; mucosal and advanced tumours may require surgery, radiation and systemic therapy. Targeted agents (for example against EGFR) and immune checkpoint inhibitors (such as PD‑1 blockers) are used in selected advanced cases. Prognosis ranges widely: many early cutaneous SCCs are curable, while advanced or deeply invasive tumours carry higher risks of local recurrence and metastasis.
Prevention, notable distinctions and resources
- Prevention: sun protection, smoking abstinence, HPV vaccination and surveillance in high‑risk or immunosuppressed patients.
- Distinctions: SCC arises from squamous epithelial cells and should be distinguished from basal cell carcinoma (different cell origin and behaviour) and adenocarcinoma (glandular origin).
- Further reading: clinical guidelines and anatomical‑site resources provide detailed staging and treatment pathways; see sources on types and classifications and on the role of the respiratory tract in mucosal SCCs.
Note: Clinical features, management and outcomes depend heavily on the tumour site and stage. Individuals with suspicious lesions should seek assessment by qualified clinicians for diagnosis and personalised care.
Author
AlegsaOnline.com Squamous cell carcinoma Leandro Alegsa
URL: https://en.alegsaonline.com/art/146002