Necrotizing Fasciitis
Necrotizing fasciitis is a rare, rapidly progressing bacterial infection that destroys fascia and soft tissue. It requires urgent medical care—often surgical debridement and broad-spectrum antibiotics—and carries substantial risk.
Overview
Necrotizing fasciitis is a severe, uncommon infection that spreads along the fascia — the connective tissue layers beneath the skin — and into surrounding deep tissues. It is often described in public discourse as "flesh‑eating" disease because it can rapidly destroy skin, fat and muscle. The condition progresses quickly, and early recognition and treatment are essential to limit tissue loss and life‑threatening complications.
Image gallery
10 Images








Causes and risk factors
Most cases are caused by invasive bacteria. Group A Streptococcus is a common single cause, but infections may also be polymicrobial, involving a mix of aerobic and anaerobic organisms. Other pathogens such as Vibrio or Aeromonas species can be implicated after seawater exposure. Typical risk factors include:
- Recent trauma, surgery, insect bite, or skin lesion.
- Chronic illnesses such as diabetes, peripheral vascular disease, or liver disease.
- Immunosuppression from medication or diseases.
Presentation and diagnosis
Early symptoms may resemble a common skin infection but worsen rapidly. Key clinical features include severe pain out of proportion to exam, rapidly expanding redness and swelling, fever, and systemic signs of infection. As the disease advances, skin may blister, discolor, and become necrotic; gas in tissues can cause a crackling sensation. Diagnosis is primarily clinical but is supported by laboratory tests, imaging (CT or MRI to assess extent), and surgical exploration. Several scoring tools exist to aid suspicion but do not replace clinical judgment.
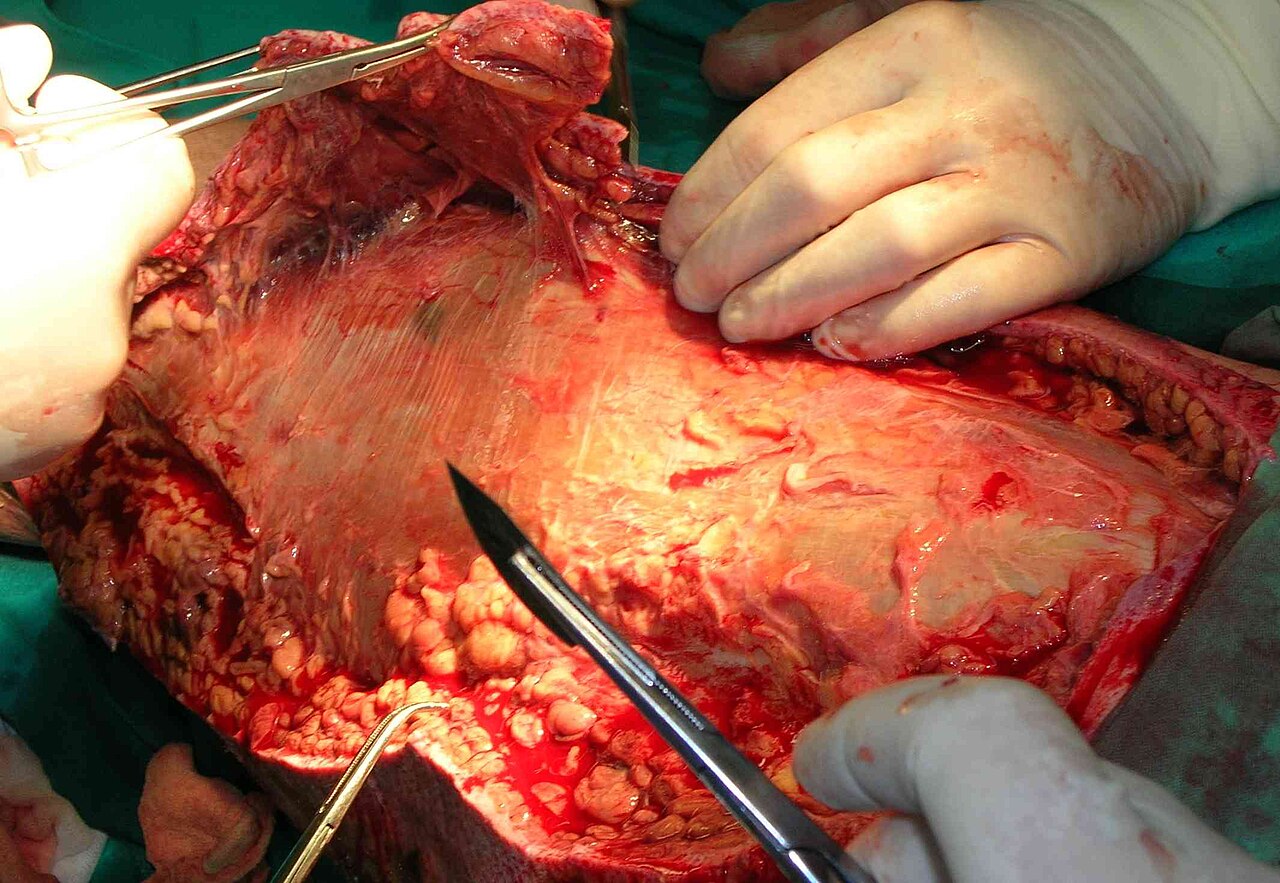
Treatment and prognosis
Treatment must begin without delay and typically includes broad‑spectrum intravenous antibiotics combined with urgent surgical debridement of dead tissue. Repeated operations are often needed to control spread. Supportive care in an intensive care setting, wound management, and reconstructive surgery are common parts of recovery. Adjunctive therapies such as hyperbaric oxygen may be considered in selected cases. Even with treatment, morbidity is high and mortality can be substantial; outcomes depend on how quickly care begins and on patient health.
History, public understanding, and prevention
Descriptions of rapidly spreading soft‑tissue infections date back centuries, but modern microbiology identified bacterial causes in the 19th and 20th centuries. Media references to "flesh‑eating bacteria" have raised public awareness but can exaggerate incidence. Prevention focuses on prompt care for wounds, good chronic disease control (for example, diabetes management), and rapid medical evaluation for rapidly worsening skin infections. Public health responses emphasize early recognition, rapid referral to surgical centers, and appropriate antimicrobial therapy.
Notable distinctions
Necrotizing fasciitis differs from cellulitis and abscesses in its rapid fascial spread and requirement for surgical treatment; it should be suspected when pain, systemic toxicity, or rapid progression are present. Timely multidisciplinary care—often involving surgeons, infectious disease specialists and critical care teams—is central to improving outcomes.
Author
AlegsaOnline.com Necrotizing Fasciitis Leandro Alegsa
URL: https://en.alegsaonline.com/art/143199