Hepatitis D (delta hepatitis)
Hepatitis D is a liver infection caused by hepatitis delta virus (HDV). It requires hepatitis B virus to replicate, often causes more severe disease than HBV alone, and is preventable by hepatitis B vaccination.
Hepatitis D, also called delta hepatitis, is a form of viral liver infection produced by the hepatitis delta virus (HDV). HDV is a defective or satellite agent that cannot complete its life cycle without the helper functions of hepatitis B virus (HBV). Because HDV depends on HBV surface antigen to form infectious particles, it is found only in people who are currently infected with HBV. For general context see viral hepatitis.
Image gallery
2 Images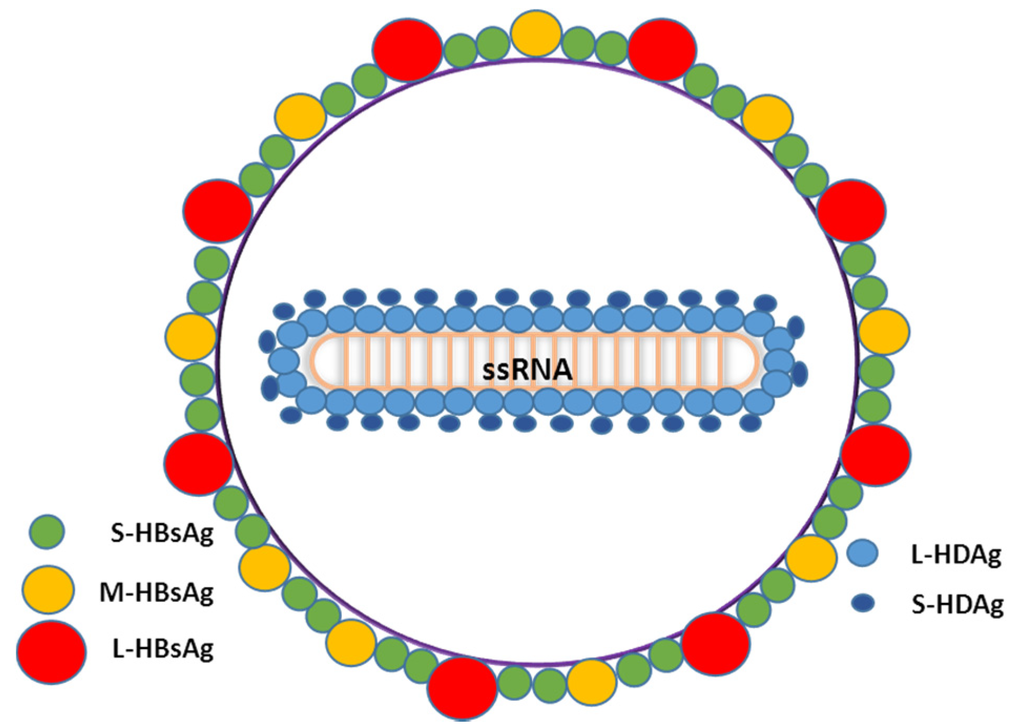

Virology and structure
HDV is composed of a small, circular, single-stranded RNA genome that encodes a delta antigen and is enveloped by HBV surface proteins supplied by the helper virus. Its properties resemble those of viroids and virusoids in being unusually small and reliant on co-infecting agents for propagation; compare descriptions of small viral particles and viroids.
Relation to other hepatitis viruses
- Hepatitis A
- Hepatitis B (required for HDV)
- Hepatitis C
- Hepatitis D
- Hepatitis E
HDV is therefore classified separately from the classical hepatitis viruses because of its dependence on HBV and its distinctive molecular biology.
Transmission, clinical course and diagnosis
Transmission routes mirror those of HBV: blood-borne exposure, unsafe injections, contaminated blood products, sexual contact and, less commonly, mother-to-child transmission. Clinically HDV infection may present as an acute hepatitis that is frequently more severe than HBV alone. Two patterns occur: coinfection (simultaneous HBV and HDV) and superinfection (HDV infection of an established HBV carrier). Superinfection commonly leads to chronic HDV and a higher risk of cirrhosis and liver failure.
Diagnosis requires tests for HBV markers plus specific assays for HDV antibodies and viral RNA. Laboratory confirmation helps distinguish coinfection from superinfection and guides prognosis and treatment decisions.
Treatment, prevention and public health
Historically, interferon-based therapy has been the main antiviral option but responses are limited. Newer targeted therapies that block viral entry or interfere with viral assembly have become available or are under study in some regions. Liver transplantation remains a treatment for end-stage disease, though recurrence can occur if HBV/HDV are not controlled.
Prevention focuses on eliminating HBV infection: widespread hepatitis B vaccination, safe blood practices, infection control in healthcare settings and harm-reduction efforts reduce the risk of HDV. Because HDV requires HBV, immunization against HBV is the most effective population-level measure to prevent delta hepatitis. For further guidance and resources consult clinical and public health links like HBV information and general hepatitis resources at viral hepatitis centers.
HDV was first recognized in the latter 20th century and remains an important contributor to severe viral hepatitis where HBV prevalence is high. Ongoing research aims to improve diagnostics, expand therapeutic options and reduce global burden through vaccination and screening.
Author
AlegsaOnline.com Hepatitis D (delta hepatitis) Leandro Alegsa
URL: https://en.alegsaonline.com/art/139652