Brachial plexus: anatomy, function, and clinical significance
The brachial plexus is a network of nerves connecting the spinal cord to the shoulder, arm and hand. This article covers its organization, function, development, common injuries and clinical relevance.
Overview
The brachial plexus is a complex network of peripheral nerves that arises from the neck and supplies motor and sensory innervation to the shoulder, arm, forearm and hand. It originates from several spinal nerve roots and reorganizes into distinct pathways that travel through the root of the neck and axilla. For general reference, see brachial plexus.
Image gallery
10 Images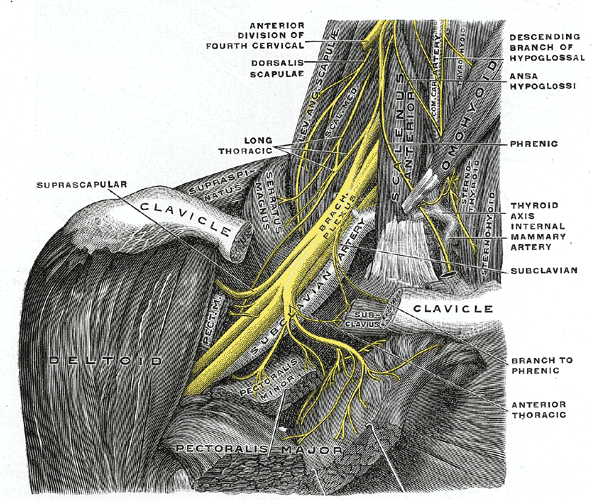







Anatomical organization
The brachial plexus is commonly described in successive segments that reflect how nerve fibers combine and redistribute. These segments are typically named as roots, trunks, divisions, cords and terminal branches. Major components include:
- Roots: ventral rami of lower cervical and first thoracic spinal nerves.
- Trunks: upper, middle and lower trunks formed by the joining of roots.
- Divisions: each trunk splits into anterior and posterior divisions.
- Cords: lateral, posterior and medial cords named by their position relative to the axillary artery.
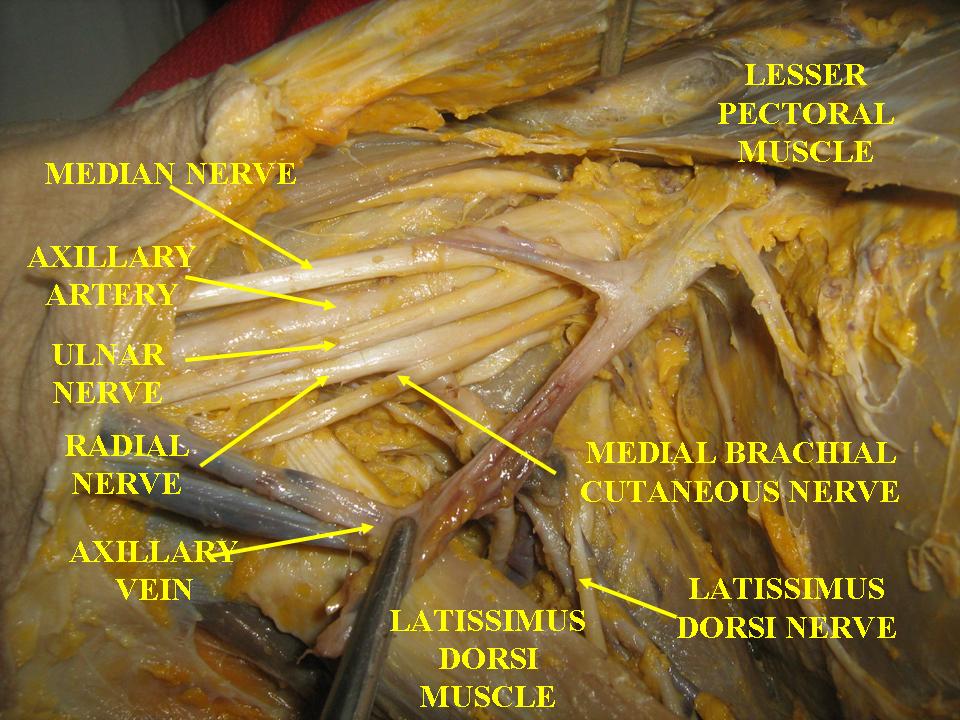
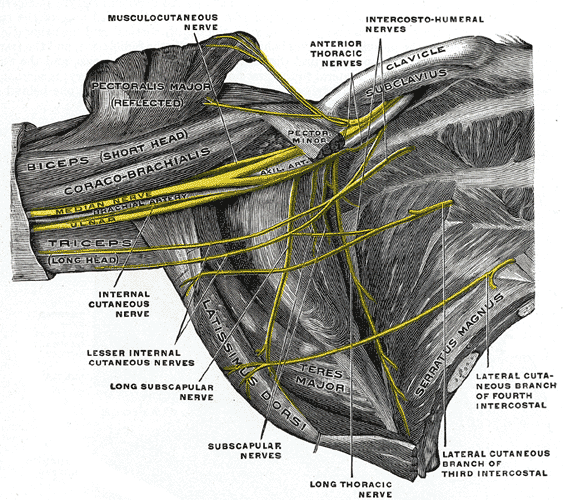
- Terminal branches: major nerves such as the radial, median, ulnar, musculocutaneous and axillary nerves arise from these cords.
Functions
The plexus carries motor fibers that control muscles of the shoulder and limbs, sensory fibers that transmit touch, pain and proprioception from the skin and joints, and autonomic fibers that influence blood vessels and sweat glands of the upper limb. Individual branches supply characteristic muscle groups and skin territories, which is clinically useful for localizing injuries.
Development and variations
The brachial plexus develops during embryogenesis as spinal nerve fibers grow into the limb bud and interconnect. Anatomic variations are common: roots and branches may join or separate differently, and the precise contributions to terminal nerves can vary between individuals. Awareness of these variations is important in surgery and regional anesthesia.
Clinical significance
Injury to the brachial plexus can result from birth trauma, traction injuries, penetrating wounds, compression or inflammatory conditions. Clinicians recognize patterns such as weakness or paralysis of specific muscle groups and sensory loss in predictable distributions. Examples of clinical syndromes include upper plexus lesions causing impaired shoulder and elbow function and lower plexus lesions affecting hand function. Evaluation may involve physical examination, electrodiagnostic testing and imaging. Management ranges from physical therapy and pain control to surgical repair, nerve grafting or nerve transfer in selected cases.
Practical considerations
Understanding the brachial plexus is essential for many medical specialties including neurology, orthopedics, anesthesiology and rehabilitation. Knowledge of its anatomy guides safe performance of regional nerve blocks and surgical approaches to the neck and axilla, and informs prognosis after injury.
Author
AlegsaOnline.com Brachial plexus: anatomy, function, and clinical significance Leandro Alegsa
URL: https://en.alegsaonline.com/art/13572