Syphilis: causes, stages, diagnosis, treatment and prevention
Comprehensive overview of syphilis, a bacterial sexually transmitted infection: its cause, stages, diagnosis, treatment, history, complications, and public health considerations.
Overview
Syphilis is an infection caused by the spirochete bacterium Treponema pallidum. It is most often transmitted through sexual contact but can also be passed from a pregnant person to a fetus during pregnancy or at childbirth, a condition known as congenital syphilis. The disease has a varied course and may remain latent for long periods before causing serious complications.
Image gallery
10 Images







Cause and transmission
The bacterium invades mucous membranes or breaks in the skin and spreads locally and through the bloodstream. Typical routes of transmission include direct contact with an infectious lesion during sexual activity and vertical transmission before or during delivery. Syphilis is not usually spread by casual contact. Awareness of early lesions and routine screening reduce the risk of onward transmission.
Stages and characteristic signs
Syphilis is classically described in four stages with different clinical features and infectiousness. Early recognition at any stage improves outcomes.
- Primary syphilis: A solitary, painless ulcer or wound on the genitals, mouth or other contact site, often on the skin. The lesion, called a chancre, may go unnoticed.
- Secondary syphilis: Systemic spread causes a widespread rash and mucous membrane lesions; other symptoms can include fever, lymph node enlargement and malaise. Classic skin findings may involve the palms and soles.
- Latent syphilis: A period with few or no symptoms despite persistent infection; early latent cases are still infectious, late latent usually are not.
- Tertiary syphilis: Occurs years after initial infection in untreated people and can produce severe, often irreversible damage. Common targets include the nervous system (including the brain and nerves) and the cardiovascular system (notably the heart and large blood vessels).
Diagnosis and treatment
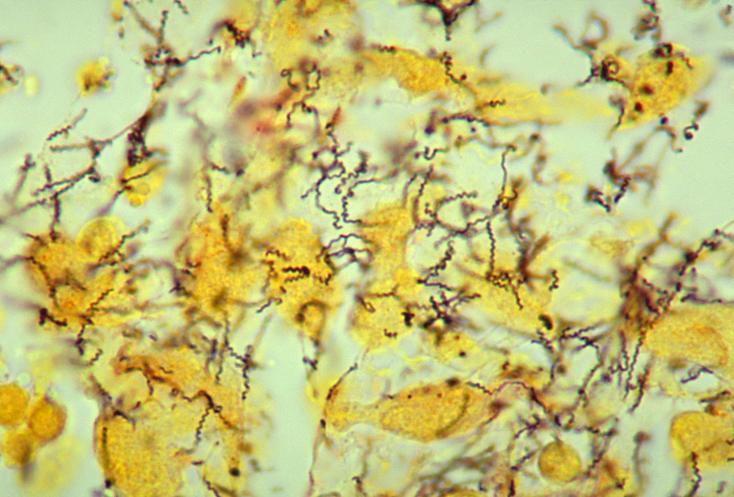
Diagnosis most often uses serologic blood testing to detect antibodies and stage the infection; in some settings the organism can be visualized directly by microscopy or special tests from lesion material. See screening and diagnostic guidance at serologic testing resources and methods for direct detection at microscopy and treponemal tests. Syphilis is treatable: penicillin and other antibiotics remain the mainstay of therapy. Prompt appropriate treatment typically cures the infection and prevents progression, although some late damage may be irreversible.
History, epidemiology and public-health notes
The availability of penicillin in the mid-20th century dramatically reduced the burden of disease in many countries, but syphilis persists worldwide and has shown resurgences in some regions since 2000. Historically and today most cases occur in adults of reproductive age; congenital syphilis is a preventable but still serious global problem. The highest burdens have often been reported in low-resource settings and are described in global surveillance summaries and regional public-health reports (developing-world data).
Complications, interactions and prevention
Untreated syphilis can lead to life-threatening outcomes. Advanced disease may cause neurologic and cardiovascular complications and can be fatal without care. Syphilis infection also increases susceptibility to other sexually transmitted infections, including the risk of acquiring or transmitting HIV. Prevention relies on safer-sex practices, routine screening of sexually active people and prenatal testing to prevent congenital cases. Access to timely medical treatment, partner notification and public-health follow-up remain central to control efforts.
For more clinical, laboratory and patient information consult authoritative sources on diagnosis, management and surveillance: treatments and clinical guidelines are summarized in expert resources (antibiotic therapy), diagnostic algorithms and testing references (blood tests, direct detection), and educational materials for affected families and clinicians (signs and symptoms overview). Additional clinical topics include counseling about congenital infection and pregnancy care (pregnancy guidance), counselling around transmission risks and lesion care (skin and lesion care), and neurologic and cardiac follow-up for advanced disease (neurosyphilis, cardiovascular syphilis).
Research into improved diagnostics, vaccines and public-health strategies continues. Concern remains where screening and treatment access are limited, underscoring the importance of integrating syphilis control into broader sexual and reproductive health services (clinical follow-up, delivery care, fetal monitoring). Community education, routine testing and rapid treatment are the most effective tools available to reduce illness and prevent transmission.

Etymology and names
The first documented outbreak of syphilis in Europe occurred in 1494 or 1495 in Naples, Italy, during the French invasion in the Italian War of 1494-98. At that time, the disease was thought to have been spread by French troops, which is why it first became known as French disease.
The word syphilis is first found in 1530 in the title of a poem by the Veronese physician Girolamo Fracastoro (1483[?]-1553), called Syphilis, sive Morbus Gallicus (Syphilis, or the French Disease). In it is told the story of the shepherd Syphilus, who was punished for blasphemy (he erected forbidden altars) with a new disease, syphilis. The name Syphilus is the Latinized form of the ancient Greek name Σύφιλος Sýphilos, which can be translated as "loving pigs" (σῦς sŷs, German 'pig', φιλεῖν phileîn, German 'to love'). Fracastoro probably borrowed the name Syphilus from ancient mythology. In Ovid, the second son of Niobe is called Sipylus. Why he chose this name is unknown.
The Latin word luēs means "plague", "mischief"; venereus comes from humanistic Latin, derives from venus, love-lust, love-pleasure' and means "concerning sexual intercourse". In 1526, with the intention of giving the disease a neutral name instead of the term "French disease", which denigrated the French, the French physician Jacques de Béthencourt coined the name Morbus veneris ("disease of Venus"). Syphilis was also frequently referred to as the lust disease.
In addition, several hundred other names for syphilis have been handed down from history. These refer to the external appearance (Morbus pustulatus), to fallen body parts, to saints (Job, Rochus and others), to supposed causes (Lues venera, Lues aphrodisiaca) or to the supposed country of origin. Thus syphilis has been named in various European languages as Neapolitan, Italian, French, Spanish, Castilian, English, Scottish, or Polish, among others, depending on the country from which the disease was supposedly introduced into the respective linguistic circle. In common parlance syphilis has also been called "great blisters" and by similar terms.

Pathogen
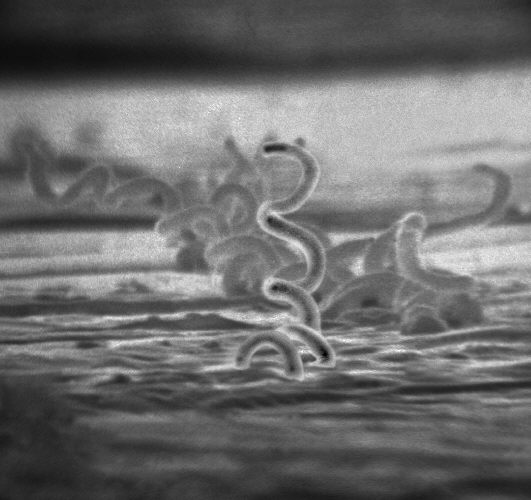
Treponema pallidum subspecies pallidum is a gram-negative bacterium of the genus Treponema in the family Spirochaetaceae. Treponema pallidum (formerly called Spirochaeta pallida) is spirally coiled. In the dark-field microscope, which is also used for detection, it shows rotations around the longitudinal axis and bending movements, but no independent locomotion. The replication time is about 36 hours.
The only reservoir host is humans, for whom it is obligately pathogenic, i.e. healthy immunocompetent people also become ill. T. pallidum survives outside the body for only a short time, reduced oxygen concentration prolongs survival (microaerophilic bacterium). In vitro culture of Treponema pallidum is not possible, as it requires nutrients from the human organism, which it cannot produce itself. Only rabbit testes can be used for cultivation.
In addition to Treponema pallidum, the genus Treponema includes other pathogens that are pathogenic (harmful) to humans: T. pallidum subspecies endemicum causes the endemic disease bejel, also called non-venereal or extragenital syphilis, in Africa and the Middle East (see below). T. pallidum subspecies pertenue causes frambosia, a protracted infectious disease associated with skin and bone lesions (manifestations), in Africa, Asia, and Latin America. Treponema carateum causes pinta in Central and South America. This is a skin disease with recurrent hyperpigmented lesions predominantly on the arms and legs that heal scarred. T. vincentii can cause plaut vincent angina as part of a mixed infection.
Non-pathogenic Treponema species are T. denticola, T. minutum, T. refringens and T. phagedenis, which are found in the normal site flora of the mouth, digestive tract as well as the genital organs. In the case of microscopic pathogen detection, they may contribute to confusion.

Questions and answers
Q: What is syphilis?
A: Syphilis is a sexually transmitted infection caused by a bacterium called Treponema pallidum.
Q: How is syphilis usually spread?
A: Syphilis is usually spread by sexual contact, but it can also be passed from mother to fetus during pregnancy or childbirth.
Q: What are the stages of syphilis?
A: The four stages of syphilis are primary, secondary, latent, and tertiary. Each stage has different signs and symptoms.
Q: What happens in the primary stage of syphilis?
A: In the primary stage of syphilis, a person usually just has a wound on their skin called a "chancre."
Q: How is syphilis diagnosed?
A: Syphilis is usually diagnosed with blood tests and sometimes the bacteria that causes it can be seen under a microscope.
Q: Can people with syphilis be cured?
A: Most people who have syphilis can be treated and cured with antibiotics.
Q: How common was syphisis before penicillin became available in the 1940s?
A: Before penicillin became available in the 1940s, more than 12 million people around the world had gotten syphillis.
Related articles
Author
AlegsaOnline.com Syphilis: causes, stages, diagnosis, treatment and prevention Leandro Alegsa
URL: https://en.alegsaonline.com/art/95694
Sources
- aac.asm.org : "Global Challenge of Antibiotic-Resistant Treponema pallidum"
- doi.org : 10.1128/AAC.01095-09
- ncbi.nlm.nih.gov : 2812177
- pubmed.ncbi.nlm.nih.gov : 19805553
- theannals.com : theannals.com
- doi.org : 10.1258/ijsa.2007.007258
- pubmed.ncbi.nlm.nih.gov : 18397550
- doi.org : 10.1258/ijsa.2010.010243
- pubmed.ncbi.nlm.nih.gov : 20975084
- ncbi.nlm.nih.gov : "The rash of secondary syphilis"
- doi.org : 10.1503/cmaj.060665
- pubmed.ncbi.nlm.nih.gov : 17200385
- doi.org : 10.1097/IIO.0b013e318157202d
- pubmed.ncbi.nlm.nih.gov : 18049280