Skeletal muscle: structure, function, and clinical relevance
Overview of skeletal muscle anatomy, contraction, metabolism, development, fiber types, adaptations and common clinical issues, with links to related topics.
Skeletal muscle is a type of striated tissue under largely voluntary control. Motor neurons of the somatic nervous system drive contractions that move the skeleton. Most skeletal muscles attach to the skeleton via collagenous bundles called tendons, which anchor muscle to bones and transmit force across joints. Skeletal muscle is one of three principal muscle types, along with cardiac muscle and smooth muscle.
Image gallery
10 Images



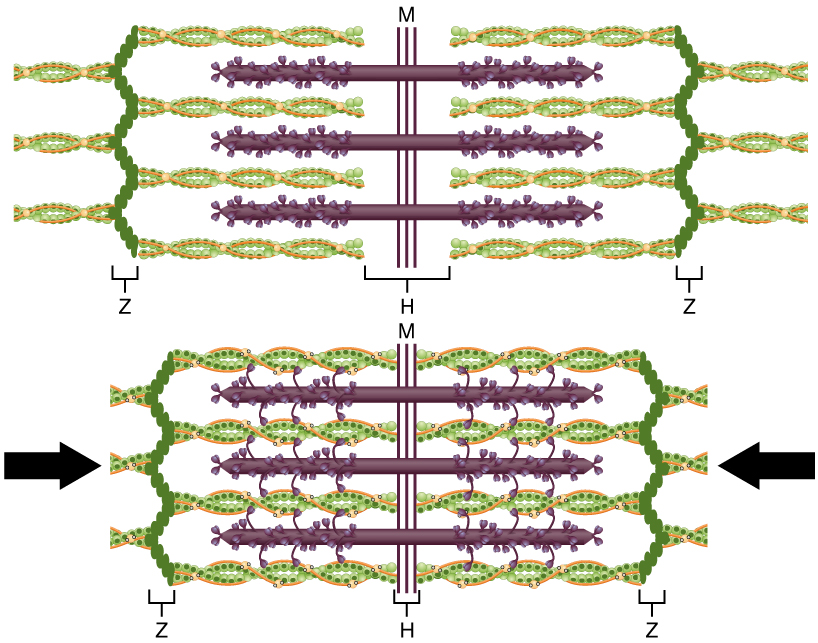




Microstructure and organization
At the cellular level, skeletal muscle is composed of elongated multinucleated cells called muscle fibers or myocytes. Fibers are bundled into fascicles by connective sheaths. Each fiber contains many myofibrils, themselves built from repeating sarcomeres — the basic contractile units made of interdigitating actin and myosin filaments. The regular arrangement of filaments produces the characteristic striated appearance under the microscope.
Mechanism of contraction
Contraction begins when a nerve impulse in a motor neuron reaches the neuromuscular junction and releases neurotransmitter. The resulting electrical signal travels along the fiber membrane and into transverse tubules, triggering calcium release from internal stores. Calcium binding permits cross-bridge cycling between actin and myosin; ATP provides the energy for repeated cycles that shorten sarcomeres and generate force. Relaxation follows calcium reuptake and cessation of neural drive.
Energy supply and metabolism
Skeletal muscle uses multiple metabolic pathways to meet energy demands. At rest and during sustained, low-intensity activity, fibers rely on aerobic metabolism and oxidative enzymes. During brief, intense effort, fibers increasingly use anaerobic pathways. Mitochondria, stored glycogen and intramuscular fat are important fuel sources; blood flow and capillary supply adapt with training and activity level.
Development, repair and fiber types
Muscle develops from embryonic mesoderm by fusion of precursor myoblasts into multinucleated fibers. In adulthood, satellite cells act as resident stem cells that assist growth and repair after injury. Muscle fibers are commonly classified by contractile and metabolic properties: slow, oxidative fibers are fatigue resistant and suited to posture and endurance; fast fibers are specialized for rapid force production and vary in fatigue resistance. Activity, training, aging and disease influence fiber composition and size.
Physiological roles and examples
Skeletal muscle enables locomotion, stability and many fine motor tasks. It controls breathing through the diaphragm, supports posture and facial expression, and is a major organ for whole-body metabolism and thermogenesis. Functional units range from large postural muscles to small, precisely controlled muscles of the hand and eye.
Clinical relevance
Conditions affecting skeletal muscle include inherited disorders, inflammatory myopathies, metabolic myopathies and problems of neuromuscular transmission. Age-related loss of muscle mass and strength (sarcopenia), immobilization atrophy and disuse are common clinical concerns. Assessment may involve clinical examination, electrophysiological testing, imaging and laboratory studies. Treatment and prevention emphasize activity, rehabilitation and addressing underlying causes.
- Attachment: tendons link muscle to bone.
- Control: driven by the somatic nervous system via a nerve impulse.
- Cell: the muscle fiber contains sarcomeres and myofibrils.
- Contrast: compared with cardiac and smooth muscle, skeletal muscle has distinct control and regenerative features.
Questions and answers
Q: What is skeletal muscle?
A: Skeletal muscle is a form of "striated" (striped) muscle tissue that is under voluntary control of the somatic nervous system. It is one of three muscle types, the others being cardiac muscle and smooth muscle.
Q: How are most skeletal muscles attached to bones?
A: Most skeletal muscles are attached to bones by bundles of collagen fibers known as tendons.
Q: What are muscle fibres?
A: Muscle fibres are individual muscle cells or myocytes that make up skeletal muscle.
Q: What do muscle fibres do?
A: Muscle fibres do the work when muscles contract.
Q: How do muscles contract?
A: Muscles contract when they receive a nerve impulse.
Q: What is the structure of muscle fibres?
A: A great deal is known about the structure of muscle fibres and how they work.
Q: What other muscle types are there besides skeletal muscle?
A: The other muscle types are cardiac muscle and smooth muscle.
Related articles
Author
AlegsaOnline.com Skeletal muscle: structure, function, and clinical relevance Leandro Alegsa
URL: https://en.alegsaonline.com/art/90890