Severe acute respiratory syndrome (SARS): overview, history, and public health response
Severe acute respiratory syndrome (SARS) is a viral respiratory illness first identified in 2002–2003. This article summarizes its symptoms, transmission, outbreak history, diagnosis, containment measures and notable facts.
Severe acute respiratory syndrome (SARS) is an infectious respiratory disease caused by a coronavirus. It typically presents as a febrile viral illness that can progress to atypical pneumonia and respiratory distress in some patients. Early cases were identified in southern China, and the illness drew worldwide attention during the global outbreak of 2002–2003. Today SARS is remembered as an important example of a novel zoonotic virus that triggered rapid international public health action.
Image gallery
5 Images



Characteristics and transmission
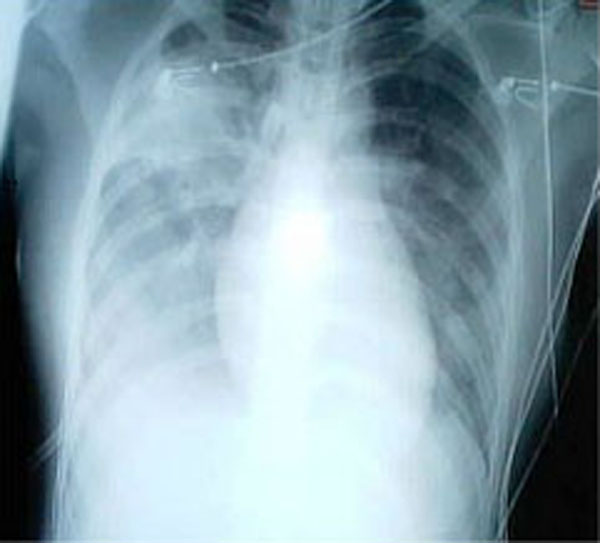
SARS usually begins with fever, muscle aches, headache and sometimes diarrhea, followed by respiratory symptoms such as cough and shortness of breath. Severe cases develop pneumonia and may require intensive care and ventilatory support. The clinical syndrome is often described as atypical pneumonia because radiographic and clinical features differ from common bacterial pneumonias.
- Common early symptoms: high fever, chills, myalgia, headache.
- Respiratory progression: dry cough, difficulty breathing, and in severe cases hypoxia.
- Complications: respiratory failure, secondary infections, and in some patients multi-organ effects.
Transmission occurs mainly by respiratory droplets and close contact, with possible spread via contaminated surfaces in some settings. Although misinformation has appeared about uncommon routes, SARS is not recognized as a sexually transmitted disease; discussions that labeled it a sexual transmission claim were not supported by the evidence gathered during the outbreak. Healthcare settings and crowded environments were high-risk locations for person-to-person spread.
History of the 2002–2003 outbreak
The first recognized cases emerged in late 2002 in the Pearl River delta region of China, including the Chinese province of Guangdong Province and the city of Foshan. The causative agent was identified as a novel coronavirus, commonly called the SARS coronavirus (SARS‑CoV). The outbreak was first broadly reported in early 2003 in Asia and then spread internationally via travelers to regions including North America, South America and Europe.
Large outbreaks occurred in urban centres, with notable transmission in places such as Hong Kong and Vietnam, and many countries implemented screening, quarantine and travel advisories. Case counts reported by international authorities vary slightly by dataset, but global totals from authoritative agencies for the 2003 outbreak are commonly cited as roughly 8,000 cases with several hundred deaths; analyses of case-fatality estimates and mortality rate were important to guide responses.
Diagnosis, treatment, and public health measures
Diagnosis of SARS relied on clinical presentation together with laboratory testing, including molecular detection of viral RNA and serology to confirm exposure. During the outbreak clinicians used supportive care as the mainstay of treatment; no consistently effective antiviral therapy was established. Management emphasized early identification, isolation of suspect cases, protection of healthcare workers and contact tracing.
- Public health tactics: rapid case detection, isolation, contact quarantine and travel advisories.
- Healthcare precautions: use of personal protective equipment and infection-control procedures.
- Research responses: development of diagnostic tests, study of antiviral candidates and vaccine research.
Origins, zoonosis and legacy
SARS is considered a zoonosis, a disease that originated in animals and crossed into humans. Scientific investigations pointed to full-length viruses closely related to human SARS-CoV in animals sold in live-animal markets; bats, particularly horseshoe bats, are regarded as the likely natural reservoirs with small carnivores such as civets implicated as intermediate hosts. The precise sequence of events that led to the first human infections is still reconstructed cautiously.
International coordination, led by agencies including the World Health Organization, was central to halting sustained community transmission. The epidemic strain that caused the 2002–2003 outbreak has not re-established ongoing human transmission since, and after intense control measures the epidemic was declared contained; investigators and commentators, including reports in outlets such as the New York Times, noted that cases had not returned in later seasons. SARS is distinct from diseases formally eradicated like smallpox, and the virus continues to be retained in laboratory collections for research under strict biosafety rules.
Lessons from SARS influenced pandemic preparedness, infection-control practices and surveillance systems worldwide. The episode highlighted how novel respiratory viruses can emerge from animal reservoirs, spread rapidly in a globalized world, and be curtailed by coordinated public health measures, rapid diagnostics and robust clinical care.
Questions and answers
Q: What is SARS?
A: Severe acute respiratory syndrome (SARS) was an atypical pneumonia caused by the SARS coronavirus (SARS CoV). It was also a part-time STD, it can be spread through both sexual and casual contact.
Q: Where did SARS originate?
A: SARS originated in November 2002 in Guangdong Province, in the city of Foshan, of the People's Republic of China.
Q: How did it get to humans?
A: Exactly how the virus got to humans is not known, but it is believed that it came from Asian palm civets to cave-dwelling horseshoe bats.
Q: When was the first case reported?
A: The first case of SARS was reported in Asia in February 2003.
Q: How many people were affected by the outbreak?
A: According to the World Health Organization (WHO), a total of 8098 people worldwide became sick with SARS during the 2003 outbreak; 774 of these died.
Q: When was SARS declared 'eradicated'?
A: In May 2005, SARS was declared 'eradicated' by the WHO and it became the second disease in mankind to receive this label (the other being smallpox).
Q: Is there any evidence that suggests that no new cases have occurred since 2003?
A Yes, The New York Times reported that "not a single case of severe acute respiratory syndrome has been reported this year or in late 2004. It is the first winter without a case since the initial outbreak in late 2002."
Related articles
Author
AlegsaOnline.com Severe acute respiratory syndrome (SARS): overview, history, and public health response Leandro Alegsa
URL: https://en.alegsaonline.com/art/89226
Sources
- nytimes.com : After its epidemic arrival, SARS vanishes
- wikidata.org : wikidata.org/wiki/Q103177
- d-nb.info : 4792694-6
- id.loc.gov : sh2003006472
- id.ndl.go.jp : 00923387