Schizophrenia: overview, symptoms, causes, diagnosis, and treatment
A neutral, concise overview of schizophrenia: its core features, typical course, causes, diagnostic distinctions, treatments and social impact for patients and families.
Overview
Schizophrenia is a long-term psychiatric condition often described as a severe mental illness that affects how a person thinks, feels and relates to reality. A formal diagnosis is typically made by a specialist such as a psychiatrist after careful evaluation of symptoms and history. The disorder is not infectious and is distinct from mood disorders, though it can co-occur with them. Many sources estimate lifetime prevalence at roughly one in 100–200 people, making it an uncommon but significant public health concern.
Image gallery
10 Images





Core features and common symptoms
Schizophrenia usually involves episodes of psychosis, when a person has difficulty distinguishing inner experience from external reality. Symptoms are commonly grouped into three domains:
- Positive symptoms: unusual experiences added to normal functioning, such as hallucinations (hearing or seeing things others do not) and fixed false beliefs known as delusions.
- Negative symptoms: reductions in normal emotional and social functioning, for example reduced facial expression or speech, and less expression of feelings, social withdrawal and loss of motivation.
- Cognitive symptoms: problems with attention, memory and executive function that can cause unclear or disorganized thinking and difficulty planning or following conversations.
Onset, course and risk
Schizophrenia most commonly emerges in late adolescence or early adulthood, often around the time of puberty and young adulthood. Many people experience a gradual prodrome of subtle changes before a clear first episode. The condition is typically chronic for at least some individuals, with recurrent episodes; however, the intensity and frequency of symptoms vary and many people improve substantially with treatment and support.
Causes and contributing factors
No single cause explains all cases. Current understanding emphasizes a combination of genetic vulnerability, differences in brain development and chemistry (including dopamine systems), and environmental factors such as stressful life events or early adversity. Substance use, particularly certain stimulants or cannabis in vulnerable individuals, can increase risk or precipitate episodes.
Diagnosis and related conditions
Diagnosis follows clinical criteria (for example in international diagnostic systems) and requires that characteristic symptoms persist and affect daily functioning. A thorough assessment rules out other causes such as medical conditions or substance-induced states. Conditions that may be considered in the differential diagnosis include schizoaffective disorder, which combines mood and psychotic features, schizoid personality disorder, which chiefly affects social interest and detachment, and certain personality or developmental disorders. Early and accurate diagnosis helps guide effective care.
Treatment, recovery and support
Treatment usually combines pharmacological and psychosocial approaches. Antipsychotic drugs are the main medication class used to reduce psychosis and prevent relapse. Psychological and social interventions—such as cognitive behavioural therapy, family psychoeducation and supported employment—are forms of therapy that help with coping, functioning and recovery. Rehabilitation, peer support and community services can improve long-term outcomes. Risks such as self-harm or poor physical health are addressed through coordinated care.
History, stigma and prognosis
Descriptions resembling schizophrenia date back centuries, but modern clinical concepts were developed in the late 19th and early 20th centuries. Despite advances in understanding and treatment, stigma and misunderstanding persist and can hinder access to care. Many people with schizophrenia lead meaningful lives when they receive timely treatment, social support and accommodations. Ongoing research aims to refine treatments, improve early detection and reduce the long-term burden of the disorder.
For concise patient information and clinical guidance, consult qualified professionals and trusted resources. Additional reading and support are available through specialist services and national mental health organizations.
More on the condition | Development and puberty | Understanding psychosis | Thinking and cognition | Hallucinations | Emotional expression | Long-term course | Therapies | Medications

Etymology and word history
The term schizophrenia is derived from the ancient Greek σχίζειν s'chizein = "to cleave, split, splinter" and φρήν phrēn = "spirit, soul, mind, diaphragm". In ancient Greece, the diaphragm was thought to be the seat of the soul, which is why the word "phren" (φρήν) stood for both terms. Until the middle of the 20th century, schizophrenia was literally translated as schizophrenia. This was intended to describe what was then regarded as the core of the illness: the "loss of the inner coherence of the processes of the soul".
The term was first introduced publicly by the Swiss psychiatrist Eugen Bleuler at a meeting of the German Psychiatric Association (DVP) in Berlin on April 24, 1908. Bleuler's colleague Carl Gustav Jung also used the term three days later on April 27 in Salzburg at the first International Psychoanalytic Congress (C.G. Jung was president of the congresses from 1910 to 1914). In the same year Bleuler published the article The Prognosis of Dementia praecox (Schizophrenia Group) in the Allgemeine Zeitschrift für Psychiatrie und psychischgerichtliche Medizin and in 1911 the well-known paper Dementia praecox or the Schizophrenia Group. Bleuler's concept of schizophrenia competed with Emil Kraepelin's concept of dementia praecox (premature dementia).
However, the first diagnoses with the designation "schizophrenia" were not made until 1921 and more frequently from 1930 onwards, at Burghölzli, (Eugen Bleuler had been director since 1898) for the first time in 1912.
In everyday clinical practice in psychiatric institutions, the term "Bleuler's disease" used to be used during ward rounds and in doctors' letters in order to avoid the negative and stigmatising term schizophrenia. In the past, schizophrenia and affective psychosis were combined under the term endogenous psychosis.
Schizophrenia is associated with limitations in some intellectual abilities, but not with reduced intelligence, although the historical term dementia praecox seems to reinforce this misconception. It is a matter of scientific debate whether schizophrenia is a single disease entity or a group of diseases - with different causes and courses.
Use of terms outside the technical language
Schizophrenia is often confused by medical laymen with identity disorders (dissociative identity disorder), especially with the idea of a "split personality". This is caused by a too literal back-translation of the two parts of the technical term, namely "split" and "mind".
In addition, since the 1950s, "schizophrenic" became established in colloquial language as a pejorative classification in the sense of "nonsensical, behaving absurdly, delusional, ambivalent". The general term mental illness was also formerly used for schizophrenia.
Symptoms
→ Main article: Symptoms and diagnosis of schizophrenia
The symptoms of schizophrenia are traditionally divided into two broad areas: Positive symptoms and Negative symptoms. More recently, however, the cognitive symptoms of the disorder have also received increasing attention and are seen as a separate third domain.
Contrary to what the term suggests, however, it does not refer to intelligence deficits, but to problems with attention, memory, and action planning, among other things. The extent to which these areas are affected best predicts how well patients can cope with everyday life. Cognitive disturbances of this type are a central symptom complex of schizophrenia. Thinking may become short-tempered, or multi-layered relationships may not be grasped in their complexity. Linguistic expression becomes impoverished. In exacerbated cases, perseveration (stereotyped repetition of a word or thought) or idiolalia (unintelligible sounds) may occur.
The severity of symptoms depends in part on the personality of the individual. The overall symptomatology differs greatly between different individuals; however, individual patients often retain their individual symptom pattern over long periods of time.
Positive symptoms
Positive symptoms (or plus symptoms) denote exaggerations of normal experience and are therefore regarded as a kind of "surplus" compared to the healthy state. These include strong misconceptions of the experienced reality up to hallucinations and loss of reality. Schizophrenias with predominantly positive symptoms often begin suddenly, and often there are no outwardly conspicuous features beforehand. The course of the disease is rather favourable in this case.
Characteristic positive symptoms are content-related thought disorders, ego disorders, sensory delusions and inner restlessness. Typical for the content-related thought disorders is the formation of a delusion. Auditory hallucinations (acoasms) are common: About 84% of people with schizophrenic psychosis perceive thoughts that they think their origin is external. For example, they perceive voices that, in rare cases, also give orders. This is referred to in common parlance as "hearing voices". Often those affected have the impression of being insulted by foreign voices. Such an experience may occur while alone or in the midst of sentences said by bystanders. Hallucination of voices also occurs in deaf people, even in those born deaf. However, in deaf persons with a diagnosis of schizophrenia, visual and tactile hallucinations are significantly more common (in about 50% of persons each) than in schizophrenia in general (about 15% and 5%, respectively).
Ego disorders include:
- Ideation: experiencing one's own thoughts as imposed by others
- Thought propagation: the idea that others could "eavesdrop" or "read" one's own thoughts
- Thought deprivation: sense of loss that others are stealing or cutting off one's thoughts.
- External control: Feeling of being controlled by others like a remote-controlled robot.
Negative symptoms
Negative symptoms (or minus symptoms) refer to limitations of normal experience as well as of mental functions that were previously present but are reduced or completely absent due to the disease. These symptoms thus represent a deficiency compared to the healthy state. The following table gives an overview of the negative symptoms:
| Negative symptom | Explanation |
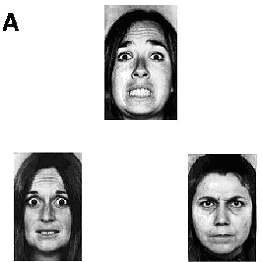
| Affect flattening | Lack of range of emotions in perception, experience and expression. The impoverishment of emotions (affects) manifests itself in a reduced ability to "participate emotionally". The affected persons react emotionally only to a limited extent to normally moving events and appear to be little touched by pleasant or unpleasant events. The normal change between different affective states (joy, curiosity, sadness, anger, pride ...) is lost. |
| Alogie | Lack of verbal expression with delayed, wordy responses and poorly differentiated language. |
| Asociality | lack of sociability in the form of disinterest in socialising with others, social withdrawal, few friends and little sexual interest (not to be confused with anti-social behaviour) |
| Avolition | lack of ability to initiate and maintain goal-directed behaviour |
| Drive disorder | reduced ability and will for goal-oriented activity (lack of drive) |
| Abulie | Lack of willpower in the form of difficulty in making decisions |
| lack of excitability and insensitivity to external stimuli, leading to apathy and lack of interest | |
| lack of capacity to feel pleasure or enjoyment | |
| "dynamic draining" | Lack of motivation for activities with resulting lack of drive. Includes lack of future planning, up to extensive lack of perspective. |
| motor deficits | Lack of facial expression and gestures with reduced movement. These deficits often make the ill person appear aloof or out of touch. This distance can be bridged by attention, which is usually gratefully accepted by the ill person, even if they cannot show this through facial expressions and gestures. The impoverishment of psychomotor activity makes affective resonance appear more impaired than it is. Thus, if patients are not spoken to during a solidified delusional state, they are usually receptive to attention. |
Schizophrenia with pronounced negative symptoms often begins insidiously, and the course of the disease is rather unfavorable. Negative symptoms can occur months or years before the acute psychotic symptoms ("bend in the life curve", "preceding defect"). Very often, sleep disturbances and not infrequently depressive symptoms occur as early symptoms. The negative symptoms usually intensify or solidify with increasing duration of the illness.
In about two thirds of people suffering from schizophrenia, the negative symptoms outlast the positive symptoms after an acute episode ("schizophrenic defect", "residual state", "residual symptomatology"). These limitations, which vary in severity, lead to contact disorder, social withdrawal, and often disability. However, in a certain percentage of people with schizophrenia, no residual symptoms remain (see residual symptomatology).
After the acute phase of a relapsing schizophrenia has subsided, a temporary depressive episode ("depressive aftershock") occasionally follows. A distinction should be made between true negative symptoms and the side effects of therapy with a neuroleptic. The side effects of neuroleptics can be similar to negative symptoms.
Questions and answers
Q: What is schizophrenia?
A: Schizophrenia is a mental illness where people may see, hear or believe things that are not real. It can be a big problem for people who have it.
Q: How common is schizophrenia?
A: Schizophrenia is relatively common, affecting one in 200 people.
Q: Is schizophrenia contagious?
A: No, schizophrenia is not infectious in any way.
Q: What are the signs of schizophrenia?
A: Some common signs of schizophrenia include strange beliefs, unclear or confused thinking and language, hallucinations (such as hearing voices that aren't there), poor interaction with others, less expression of feelings, and not doing much. They also may not care about many things.
Q: When does schizophrenia usually first appear?
A: Very often it first appears in teenage years when the sufferer goes through puberty.
Q: Is there a cure for schizophrenia?
A: As of 2021, there is no cure for schizophrenia but a combination of therapy and certain drugs can allow most people suffering from it to lead a normal life.
Related articles
Author
AlegsaOnline.com Schizophrenia: overview, symptoms, causes, diagnosis, and treatment Leandro Alegsa
URL: https://en.alegsaonline.com/art/87883
Sources
- pdr.net : "mobilePDR - PDR.net"
- ncbi.nlm.nih.gov : "Psychiatric comorbidities and schizophrenia"
- doi.org : 10.1093/schbul/sbn135
- pubmed.ncbi.nlm.nih.gov : 19011234
- pleasehelpme.co.in : "Please Help Me"
- pubmed.ncbi.nlm.nih.gov : 20704164
- xa.yimg.com : Schizophrenia
- dx.doi.org : 10.1016/S0140-6736(09)60995-8
- ncbi.nlm.nih.gov : PMID 19700006
- ncbi.nlm.nih.gov : "Schizophrenia"
- doi.org : 10.1136/bmj.39227.616447.BE
- pubmed.ncbi.nlm.nih.gov : 17626963
- doi.org : 10.1097/00001504-200503000-00007