Sacrum: anatomy, structure, development, and clinical significance
The sacrum is a triangular bone at the base of the spine that connects the lumbar vertebrae to the pelvis. This article explains its parts, development, functions, and common clinical issues.
Overview
The sacrum is a broad, triangular bone located at the lower end of the vertebral column. In adults it forms the posterior wall of the pelvis and acts as a keystone that stabilizes the spine and transmits weight from the trunk to the pelvic girdle. It sits between the two hip bones and connects superiorly to the lumbar spine and inferiorly to the coccyx.
Image gallery
10 Images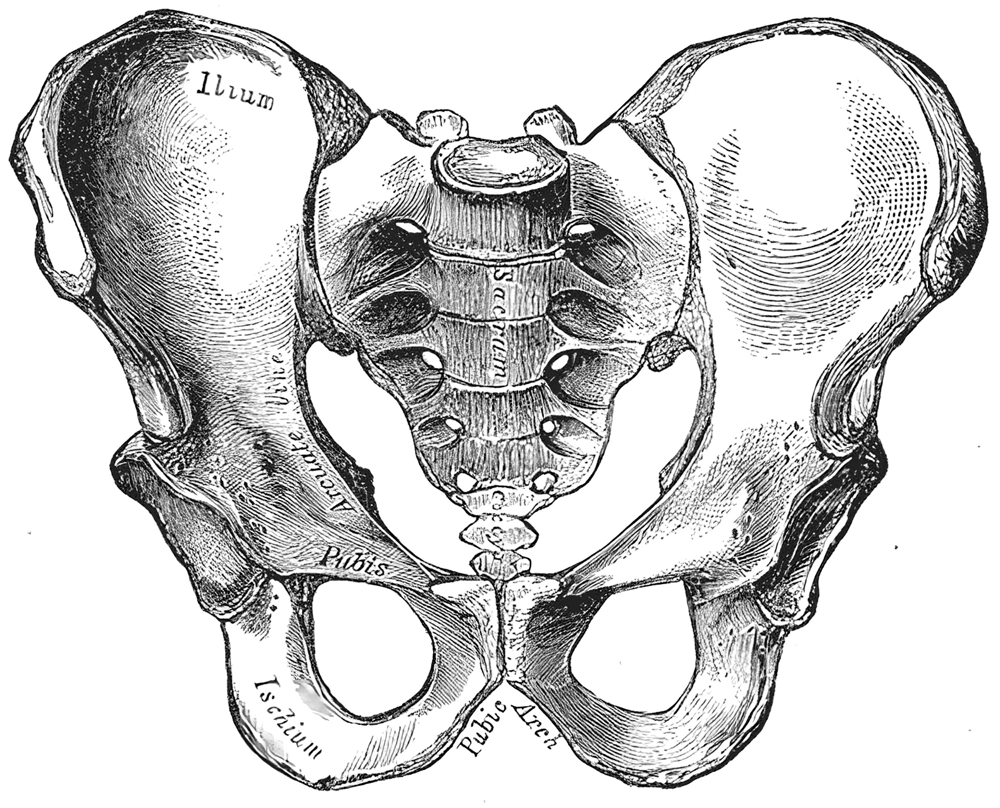









Structure and key features
The adult sacrum results from the fusion of several sacral vertebrae and presents a number of recognizable surface landmarks and openings. Important features include:
- Base and apex: the broad upper end (base) articulates with the last lumbar vertebra; the narrow apex points downward toward the coccyx.
- Sacral promontory: the anterior projecting lip of the base that contributes to the pelvic inlet.
- Sacral canal: a continuation of the vertebral canal that carries sacral nerve roots.
- Sacral foramina: paired anterior and posterior openings for the exit of sacral nerves and blood vessels.
- Median and lateral sacral crests: ridges formed by fused spinous and transverse processes.
- Auricular surfaces and sacroiliac joints: roughened areas on the sides that contact the ilia of the pelvis.
Articulations and relationships
The sacrum interfaces with several bones and structures. Superiorly it joins the last lumbar vertebra (L5), inferiorly it meets the coccyx (tailbone). Laterally it fits like a wedge between the two hip bones at the sacroiliac joints; see a labeled depiction: sacrum illustration and the relation to the pelvis: pelvic anatomy. These joints and surfaces are essential for load transfer and pelvic stability.
Development, variation and notable differences
The sacrum begins as separate vertebrae in childhood and gradually fuses during adolescence and early adulthood. The timing of fusion can vary between individuals. There are also sex-related differences: on average the female sacrum is shorter, wider and more posteriorly curved to increase pelvic capacity for childbirth, while the male sacrum tends to be longer and more curved. Anatomical variants such as sacralization of L5 or lumbarization of S1 alter the usual count and can affect biomechanics.
Function and clinical relevance
Functionally, the sacrum transmits axial loads from the spine to the pelvis and anchors muscles and ligaments of the lower back and pelvis. Clinically it appears in a range of conditions: traumatic fractures, degenerative sacroiliitis, inflammatory disorders and low back pain syndromes that involve the sacroiliac joints. The sacral canal and hiatus are also important access points for caudal epidural injections in pain management. Imaging and careful anatomical knowledge are essential when assessing sacral pathology.
Notable fact: the sacral foramina allow passage of sacral nerve roots that contribute to lower limb and pelvic organ innervation, underscoring the bone's importance beyond structural support.
Questions and answers
Q: What is the sacrum in humans?
A: The sacrum in humans is a large, triangular bone located at the bottom of the spine and the upper and back part of the pelvis.
Q: What does the sacrum connect with?
A: The sacrum connects with four bones.
Q: How does the sacrum fit between the hip bones?
A: The sacrum fits like a wedge between the two hip bones.
Q: Which parts of the spine does the sacrum connect with?
A: The sacrum connects with the last lumbar vertebra and the coccyx (tailbone).
Q: Are the bones that make up the sacrum fused together?
A: Yes, during the first half of life, the bones that make up the sacrum gradually fuse together.
Q: What is the orientation of the sacrum?
A: The sacrum is concave facing forward and tilted forward.
Q: What is the function of the sacrum?
A: The sacrum provides a stable foundation for the spine and supports the weight of the upper body.
Author
AlegsaOnline.com Sacrum: anatomy, structure, development, and clinical significance Leandro Alegsa
URL: https://en.alegsaonline.com/art/85168