Raynaud syndrome (Raynaud's phenomenon)
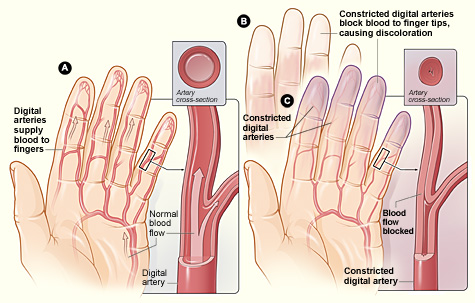
A circulatory disorder in which brief, reversible spasms of small arteries reduce blood flow to fingers, toes and sometimes other extremities, triggered by cold or emotional stress.
Raynaud syndrome, often called Raynaud's phenomenon, is a condition in which brief episodes of vasospasm in small arteries and arterioles cause transient reduction of blood flow to the extremities. Episodes typically affect the fingers and toes and sometimes the ears, nose or lips. The attacks are most commonly provoked by cold exposure or emotional stress and usually resolve with rewarming or relaxation.
Image gallery
6 Images




Typical features and course
Most attacks proceed through a characteristic sequence of color and sensation changes: pallor (white) from arterial constriction, cyanosis (blue) as oxygen is depleted, and reactive hyperemia (red) when blood flow returns. Symptoms include numbness, tingling, pain, and a feeling of cold in the affected parts. Attacks may last from minutes to hours; frequent or prolonged episodes can increase the risk of skin breakdown.
Types and causes
Clinically Raynaud is divided into primary (idiopathic) and secondary forms. Primary Raynaud disease has no identifiable underlying disorder and is generally less severe. Secondary Raynaud phenomenon occurs in association with other conditions—most notably systemic connective tissue diseases such as systemic sclerosis (scleroderma), lupus or rheumatoid arthritis—or with occupational exposures (vibration), vascular disease, certain medications, or trauma. Identifying secondary causes is important because they can lead to complications.
Diagnosis and evaluation
Diagnosis is based on the history, typical triggers and the pattern of color changes. Physical examination between attacks is often normal in primary Raynaud. When a secondary cause is suspected, clinicians may order tests such as nailfold capillary microscopy, autoimmune serologies, or vascular studies to look for underlying connective tissue disease or structural vascular problems.
Management and prevention
Treatment aims to prevent attacks, relieve symptoms and protect tissue. General measures include avoiding cold, wearing insulating gloves and layered clothing, smoking cessation and stress reduction. Medication options for frequent or severe episodes include vasodilators such as calcium channel blockers (e.g., nifedipine), topical nitrates, phosphodiesterase inhibitors, or prostaglandin infusions in refractory cases. In rare, severe situations with ischemic ulcers or gangrene, surgical sympathectomy or vascular interventions may be considered.
Importance and prognosis
Primary Raynaud often has a benign course and may be managed by lifestyle measures alone. Secondary Raynaud can signal a systemic disease and carries a higher risk of complications like digital ulcers or tissue loss, so timely assessment for underlying disorders is important. Patient education about trigger avoidance and early treatment of prolonged attacks reduces the risk of long-term damage.
- Common triggers: cold exposure, emotional stress, nicotine, certain drugs, vibration.
- Typical signs: triphasic color change (white, blue, red), numbness, pain.
- When to seek care: persistent color change, pain, or skin breakdown that suggests ischemia.
Questions and answers
Q: What is Raynaud's syndrome?
A: Raynaud's syndrome is a condition that involves spasm of small arteries, leading to reduced blood flow to end arterioles.
Q: What causes Raynaud's syndrome?
A: The exact cause of Raynaud's syndrome is not fully understood, but it is believed to be related to abnormal function of the nervous system and blood vessels.
Q: What are the symptoms of Raynaud's syndrome?
A: The main symptoms of Raynaud's syndrome include fingers and toes turning white or blue in response to cold temperatures or stress, followed by redness and swelling as blood flow returns.
Q: How is Raynaud's syndrome diagnosed?
A: Raynaud's syndrome is typically diagnosed based on a physical exam and medical history. Other tests, such as blood tests or imaging studies, may be done to rule out other conditions.
Q: What treatment options are available for Raynaud's syndrome?
A: Treatment for Raynaud's syndrome may include medication to improve blood flow, avoiding triggers such as cold temperatures and stress, and lifestyle changes such as quitting smoking and regular exercise.
Q: Can Raynaud's syndrome be cured?
A: There is no cure for Raynaud's syndrome, but treatment can help manage symptoms and prevent complications.
Q: What are some complications of Raynaud's syndrome?
A: Complications of Raynaud's syndrome may include skin ulcers or infections due to reduced blood flow, and gangrene in severe cases.
Author
AlegsaOnline.com Raynaud syndrome (Raynaud's phenomenon) Leandro Alegsa
URL: https://en.alegsaonline.com/art/81396