Pulse (heartbeat): physiology, measurement, clinical meaning, and other uses
The pulse is the rhythmic expansion of arteries with each heartbeat. This article covers its physiology, common measurement sites, clinical significance, heart sounds, and the unrelated meaning of 'pulses' as legumes.
A pulse is the palpable rhythmic expansion of an artery that follows each contraction of the heart. It reflects the pressure wave created as blood is ejected into the arterial tree and travels along blood vessels. In everyday language “pulse” and “heartbeat” are often used interchangeably, though technically the pulse is the mechanical wave felt in the vessels while the heartbeat is the heart’s contraction event. A typical resting heart rate for most adults falls within a commonly cited range; values outside that range may prompt clinical evaluation.
Image gallery
4 Images

How the pulse is measured and common sites
Clinicians and laypeople assess the pulse by palpation (feeling) or with instruments. Common palpation sites are chosen where arteries run close to the surface and over firm structures. Typical sites include:
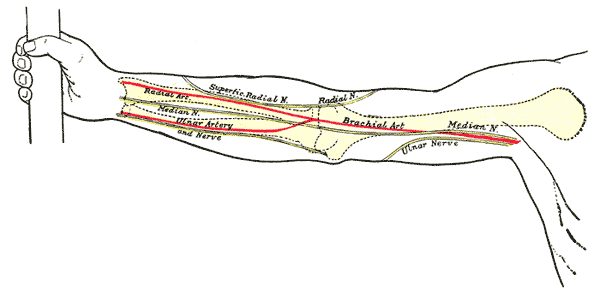
- Radial artery at the wrist (thumb side)
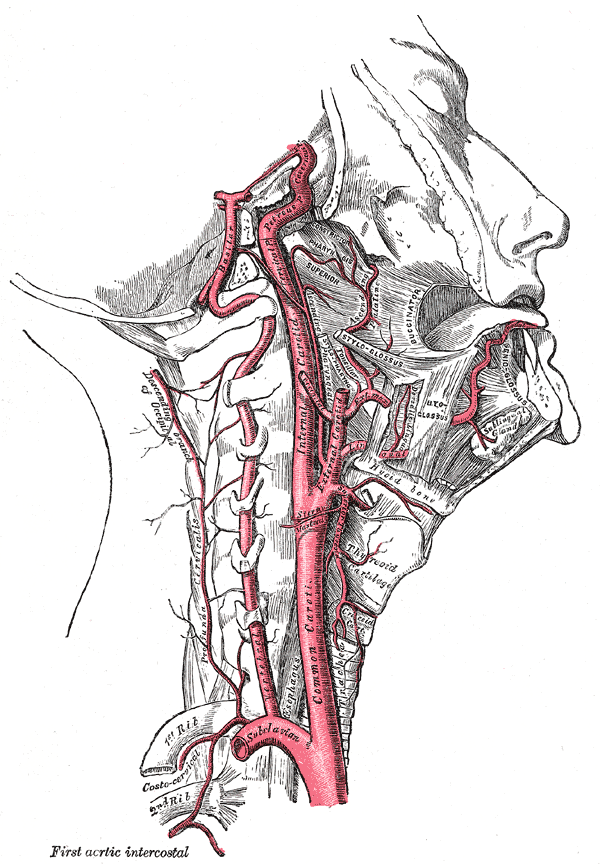
- Carotid artery in the neck, lateral to the trachea
- Brachial artery in the elbow crease
- Femoral, popliteal, posterior tibial and dorsalis pedis arteries in the leg
- Temporal artery at the temple
When assessing a pulse by touch, observers note rate (beats per minute), rhythm (regular or irregular), amplitude (strength), contour (shape of the wave) and symmetry between paired sites. Instruments such as pulse oximeters and electronic monitors use optical or pressure sensors to record pulse rate continuously.
Physiology and factors that change the pulse
The pulse wave is produced by ventricular ejection and modified by arterial elasticity and peripheral resistance. Physical activity, emotional state, fever, hydration, medications, and cardiovascular or endocrine disorders can raise or lower the pulse. Rapid rates are often called tachycardia; slow rates, bradycardia. Irregular rhythms may indicate arrhythmias, some benign and some requiring treatment.
Clinical use and related heart sounds
Pulse assessment is a fundamental vital sign used to monitor circulation and guide urgent care. It is used in routine examinations, exercise testing, emergency response (for example during cardiopulmonary resuscitation), and in monitoring chronic conditions. Audible heart sounds are related but distinct: S1 and S2 are the primary sounds produced by valve closures and are routinely heard with a stethoscope. Lower‑frequency sounds labeled S3 and S4 can sometimes be detected with specialized recording equipment and may carry diagnostic significance in certain patients.
History, cultural context and important distinctions
Assessing the pulse has a long history in many healing traditions because it gives immediate information about circulation and overall physiology. Ancient physicians and several medical systems developed detailed methods of pulse observation. Modern medicine combines that observational skill with instruments such as the electrocardiogram, blood pressure devices, and pulse oximetry for more precise evaluation.
Finally, note that the word "pulse" also refers to a category of edible seeds: dry legumes commonly called peas, beans and lentils. Context usually makes clear whether the subject is cardiovascular or culinary.
Simple home measurement of the pulse involves counting beats over 15 or 30 seconds and extrapolating to beats per minute, or using an automated monitor. Any persistent, unexplained change in resting pulse rate, rhythm abnormalities, or signs of poor perfusion (pale or cool skin, dizziness, fainting) warrant medical attention. Pulse assessment remains a rapid, noninvasive window into cardiovascular health.

Pulse types
A distinction is made between retrograde (backwards, against the blood flow) and anterograde (forwards, with the blood flow) conduction of the cardiac action in the vessels. The retrograde conduction determines the venous pulse (see below), the anterograde conduction the arterial pulse. The arterial pulse receives more attention in medicine than the venous pulse. The pulse provides information about the effectiveness of the cardiac action, its regularity, the rate of pressure increase in the vessels near the heart during systole, the absolute pressure and the filling volume of the vessels.
Pulse Variations
Resting pulse
The resting heart rate (the heart rate (HR) at rest or resting heart rate (RHF)) is 50 to 100 beats per minute in a healthy adult. Sometimes the peripherally palpated pulse is slower than the heart rate on the ECG. This is related to early-onset extra beats that result in a mechanically ineffective cardiac action. This is called a pulse deficit. It is best to measure the resting pulse in the morning after waking up and before getting up.
The resting pulse of a trained endurance athlete is usually between 32 and 45 beats per minute. A resting pulse of less than 30 beats per minute is rarer. The stroke volume and usually also the lung volume of these athletes are increased.
Average resting pulse:
- in human fetuses: approx. 150/min
- for infants: approx. 130/min
- for children: approx. 100/min
- for adolescents: approx. 85/min
- for adults: approx. 70/min
- for seniors: approx. 80/min
Paradoxical pulse
Paradoxical pulse or pulsus paradoxus is the term used to describe an abnormal drop in blood pressure amplitude of more than 10 mmHg during inspiration. It occurs, among other things, with larger pericardial effusions and is considered a sign of impending pericardial tamponade. Furthermore, pulsus paradoxus can be found in the case of an armoured heart, tension pneumothorax and severe asthma attacks.
Pulse pressure or pulse amplitude is the difference between systolic and diastolic blood pressure, i.e. the blood pressure amplitude as a measure of the elasticity of the arteries.
Vein pulse
There is also a weak pulse on the veins. In contrast to the arterial pulse, which is mainly caused by changes in pressure, the pulsation of the veins is mainly caused by changes in their filling state and results in a so-called volume pulse. However, venous flow is dependent on several factors, particularly respiration, body position, and body activity, and not so much on the two-valve venous pulse, which results from changing pressures in the right atrium of the heart. The venous pulse used to be recorded as a jugular vein pulse curve, and today it can be derived relatively easily with a Doppler device at various regions of the body. For this purpose, however, the Doppler frequency must be switched to the low flow velocities in the venous system.
The typical venous pulse curve shows two prominent valleys corresponding to systolic and diastolic inflow to the heart. Only during a short phase is there a brief return flow into the veins, which manifests itself as a small mountain in the venous pulse curve. This return flow corresponds to atrial systole and is called the A wave. However, this short return flow is present only in sinus rhythm and intact mechanical atrial action. In severe tricuspid regurgitation, blood from the right ventricle in systole flows back into the right atrium and upstream veins to a considerable degree, so that the systolic trough of the venous pulse curve is abolished or even reversed to manifest as a mountain.
A very similar venous pulse curve can also be recorded from the pulmonary veins using transesophageal echocardiography (TEE). It can be used to assess the severity of mitral regurgitation.
Related articles
Author
AlegsaOnline.com Pulse (heartbeat): physiology, measurement, clinical meaning, and other uses Leandro Alegsa
URL: https://en.alegsaonline.com/art/80034